
 Amit Patel discusses the benefits of Periochip, which helps to prevent periodontal pockets.
Amit Patel discusses the benefits of Periochip, which helps to prevent periodontal pockets.
As already reported by Chang et al (2013) osteoporosis and periodontitis are both considered international health issues. Although the association between them is still unclear, a five-year follow-up, population-based study in Taiwan indicated that patients with osteoporosis might have an increased risk of periodontitis.
Osteoporosis is a destructive skeletal disease distinguished by reduced bone mass and increased bone fragility. It is diagnosed by the measurement of bone mineral density and can occur in adults, young people and children.
By the age of around 30-years, maximum bone density and strength is achieved in humans, followed by a natural decline. Women are four times more likely to develop osteoporosis than men and their lighter, thinner bones and longer life spans are part of the reason (Pack et al, 2001). Postmenopausal women over 50 have a greater risk of developing osteoporosis and it is estimated that one in three women in this category will suffer from the condition.
Osteoporosis and periodontitis
Professor Robin Seymour, Newcastle University, was recently asked to comment on some new research by two large scale National Health Studies and noted that the studies confirmed a clear association between osteoporosis and periodontitis. He also cited that women with a history of periodontal disease or osteoporosis would most probably experience accelerated bone and tooth loss.
Professor Seymour said it would be wise for osteoporotic patients to enquire whether treatment for their condition could reduce the risk of periodontal disease and tooth loss. Studies suggest oestrogen supplementation in postmenopausal women reduces gingival inflammation and frequency of periodontal destruction (Reinhardt et al, 1999).
As well as gender, there are other factors that increase the risk of developing osteoporosis including age, family history, previous fractures, ethnicity, menopause/hysterectomy and rheumatoid arthritis. Other more modifiable causes that can also increase the risk of fracture or a decrease in bone mineral density include: alcohol, smoking, low body mass index, poor nutrition, vitamin D deficiency, eating disorders, insufficient exercise, low calcium intake and frequent falls (www.iofbonehealth.org, 2014).
Both osteoporosis and periodontal diseases are bone damaging diseases, and it has been theorised that osteoporosis could be a risk factor for the progression of periodontal disease (Darcey et al, 2013).
Extensive research into the correlation of the two diseases suggests that decreased bone mineral density due to osteoporosis can lead to a more rapid resorption of bone in the jaw. More specifically, when the alveolar or jaw section containing and supporting the tooth sockets becomes less dense, the destruction of tissue or bone around the teeth can occur leading to tooth loss (Darcey et al, 2013).
The National Institutes of Health Osteoporosis and Related Bone Diseases National Resource Center, Maryland, states that it is possible that the loss of alveolar bone mineral density leaves bone more susceptible to periodontal bacteria, increasing the risk for periodontitis and tooth loss.
The effects
Patients with osteoporosis are advised to attend six-monthly dental appointments and to request a thorough inspection of their periodontal tissues.
Patients should always be encouraged to maintain good oral care and plaque control is of paramount importance. Plaque can progressively damage teeth and the surrounding tissue and may develop into gingivitis or periodontal disease. If debris and bacteria are allowed to build up in periodontal pockets along the gingival margin, the bacterial toxins and the immune system’s response to infection begin to destroy the bone and tissue that hold the teeth in place.
When such a periodontal pocket occurs, professional cleaning is required to remove the bacteria and prevent infection. Traditionally scaling and root surface debridement are used to clean the subgingival areas. Sometimes a course of antibiotics is also required to treat infection and in more serious cases surgery may be needed due to bacterial resistance.
Treatment
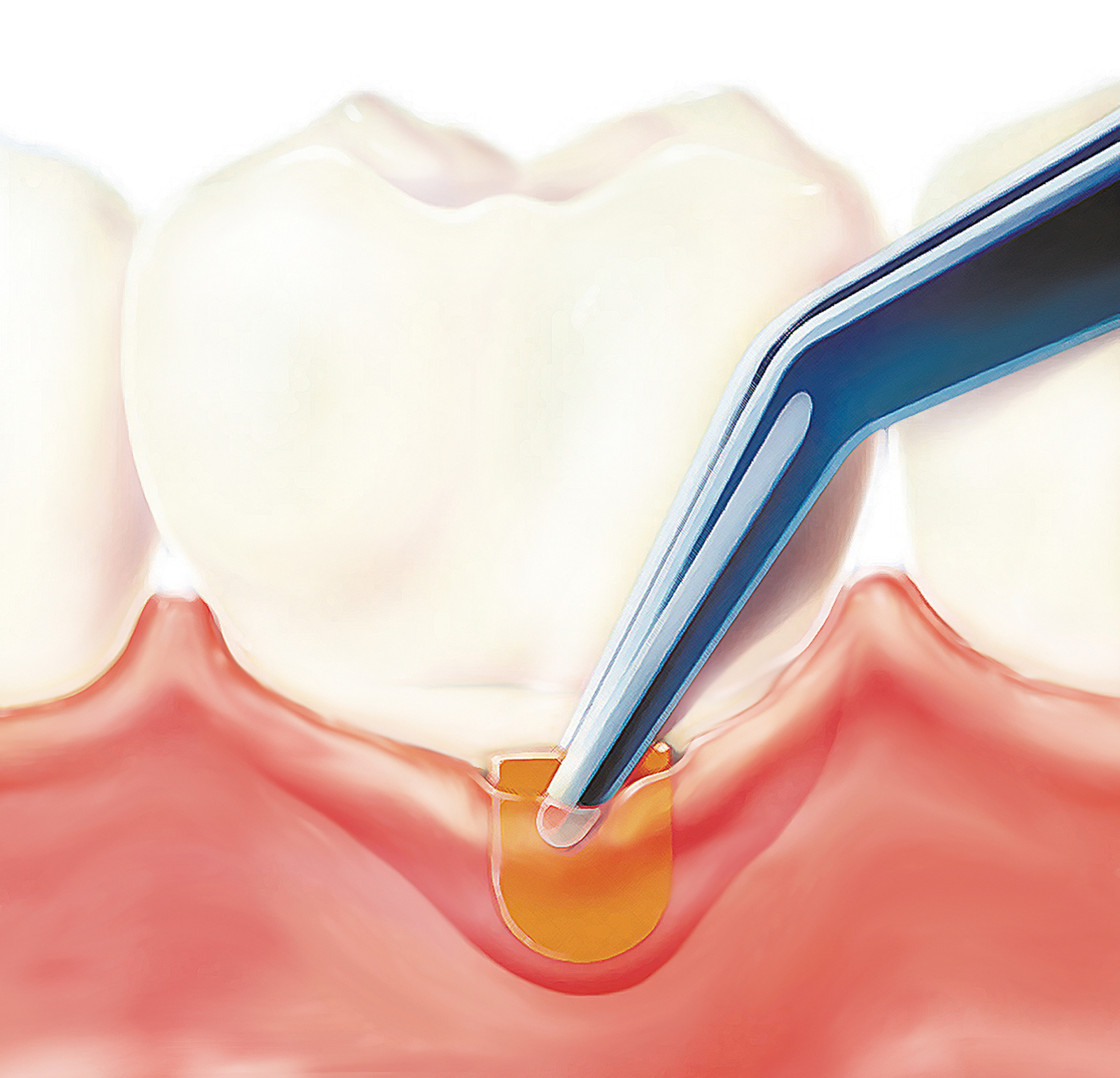
Described as a ‘first line’ treatment of periodontal pockets, a biodegradable intraperiodontal chip called Periochip is available to minimise local harmful bacteria. The gelatin-based chip is inserted into periodontal pockets where its active ingredient, chlorhexidine digluconate, is slowly released over 10 days and kills 99% of bacteria. Periochip eliminates 99% of subgingival bacteria, and suppresses the growth of bacteria for up to 11 weeks (Jeffcoat et al, 1998). Results from the clinical studies showed a pocket reduction of more than 2mm in almost three quarters of patients when placed every three months (Soslkolne et al, 2003). Periochip is an effective adjunctive treatment option for periodontal disease. Periochip does not require any special equipment to place and it takes just 30 seconds. Periochip is biodegradable and dissolves naturally over 48 hours.
As well as osteoporosis, periodontal disease has been linked to many general health problems including cardiovascular disease and diabetes Schenkein and Loos (2013) have shown. It’s therefore essential patients are provided an accurate diagnosis, quickly. Effective treatment and the prevention of bacterial toxins building up to protect the overall health of the body are crucial for all sufferers.
References
Chang WP, Chang WC, Wu MS, Pai JT, Guo YC, Chen KC, Liu ME, Chiu WT, Hung KS (2014) Population-Based 5-Year Follow-Up Study in Taiwan of Osteoporosis and Risk of Periodontitis. J Periodontology 85(3): 24-30
Darcey J, Devlin H, Lai D, Walsh T, Southern H, Marjanovic E, Horner K (2013) An observational study to assess the association between osteoporosis and periodontal disease. J British Dental 215: 617-621
Jeffcoat MK, Bray KS, Ciancio SG, Dentino AR, Fine DH, Gordon JM, Gunsolley JC, Killoy WJ, Lowenguth RA, Magnusson NI, Offenbacher S, Palcanis KG, Proskin HM, Finkelman RD, Flashner M (1998) Adjunctive use of a subgingival controlled-release chlorhexidine chip reduces probing depth and improves attachment level compared with scaling and root planning alone. J Periodontal 69(9): 989-997
Pack ARC, Francis RM, Seymour RA, Thomson WM (2001) Oral radiographic findings and skeletal bone mineral density (BMD) relationships. In: British Society for Dental Research & Irish Division: Joint Meeting. Belfast , UK: 2001, Belfast, UK. Sage Publications.
Reinhardt RA, Payne JB, Maze CA, Patil KD, Gallagher SJ, Mattson JS (1999) Influence of estrogen and osteopenia/osteoporosis on clinical parameters in postmenopausal women. J Periodontal 70: 823-8
Soslkolne WA, HM Proskin, Ayala Stabholz (2003) Probing depth changes following 2 years of periodontal maintenance therapy including adjunctive controlled-release of chlorhexidine. J Periodontology 74: 420-427
Schenkein HA, Loos BG (2013) Inflammatory mechanisms linking periodontal diseases to cardiovascular diseases. J Periodontology 40: 51-69
www.iofbonehealth.org/sites/default/files/PDFs/know_and_reduce_your_risk_english.pdf retrieved 1/8/14
For more information on Periochip email [email protected] or free phone 0800 013 233.

