 Amit Patel and Hinali Patel investigate the prescription preferences of dental practitioners for direct and indirect veneers.
Amit Patel and Hinali Patel investigate the prescription preferences of dental practitioners for direct and indirect veneers.
Abstract
Introduction: due to the increase in demand for cosmetic dentistry, researching prescription preferences of dental practitioners’ for ceramic or composite veneers will provide invaluable data on which treatment modality is favoured.
Aim: to determine the prescription preferences of dentists for composite and ceramic veneers in the UK.
Method: an online questionnaire was designed and piloted before online distribution to dentists. The survey consisted of closed questions in order to analyse the qualitative data. The results were collated, validated, analysed and discussed.
Results: a total of 418 (4.18%) responded to the survey.
Dentists preferred the use of ceramic veneers compared to composite veneers under the same clinical circumstances (p=0.000).
It was statistically significant that the number of years qualified influences the short-term complication incidence (p=0.016).
Twenty per cent of dentists are not influenced by the age of the patient when providing ceramic veneers (p=0.021).
Conclusion: these results suggest that dentists, under the same clinical circumstances, prefer to place ceramic veneers compared to composite veneers.
Introduction
In recent years, there has been an increase in ‘dental demand’ for cosmetic dentistry (Kelleher, 2010). It is estimated that around £3 billion is spent on cosmetic dentistry in the UK each year. UK expenditure can be expected to multiply in line with other countries, combined with the influence of fashion and social media on the public (Robinson, Patel and Pennycate, 2004).
Evidence surrounding the longevity of anterior composite veneers is limited. In 1999, Burke observed 9,031 restorations of which 29.8% were composite. Failure was classified into fracture, microleakage, and debonding. They found the mean survival for composite restorations was 4.5 years, but a limitation of the study was that they did not differentiate between anterior and posterior composite restorations (Burke et al, 1999).
More recent evidence in 2007 studied the long-term survival of direct composite restorations in the treatment of advanced tooth wear and found the 10-year survival for the direct composite was 58.9%. However, they only observed a minimal sample size of 17 patients (Smales and Berekally, 2007).
Direct composite veneers will not replace the well-established ceramic veneer technique. However, they are an alternative method to directly veneering or building up anterior teeth, which can be a time-consuming process (Dietschi and Devigus, 2011).
There is a lack of reliable evidence to show whether direct composite veneers outperform ceramic veneers or vice versa in terms of longevity, aesthetic outcomes and ability to repair (Wakiaga et al, 2004).
Materials and methodology
Procedure
An online questionnaire was created in Surveymonkey, which is an online survey development cloud-based software. The survey consisted of closed questions in order to analyse the qualitative data. This is a cross-sectional survey and was initially piloted in April 2019. The results of the study were collated, validated, analysed and discussed.
Participants
The survey was distributed via social media to dental practitioners currently registered with the General Dental Council (GDC). Exclusion criteria related to any dentist not registered with the GDC and therefore, overseas dentists were not allowed to participate in the study. Valid responses were received from 418 respondents (4.18%) from 31 May 2019 until 30 June 2019; all of which met the inclusion criteria. Informed consent was obtained and confidentiality was maintained for all participants.
Results
Data analysis was performed in SPSS Version 22. Descriptive statistics were used to provide meaningful descriptions of the sample data.
Material of choice
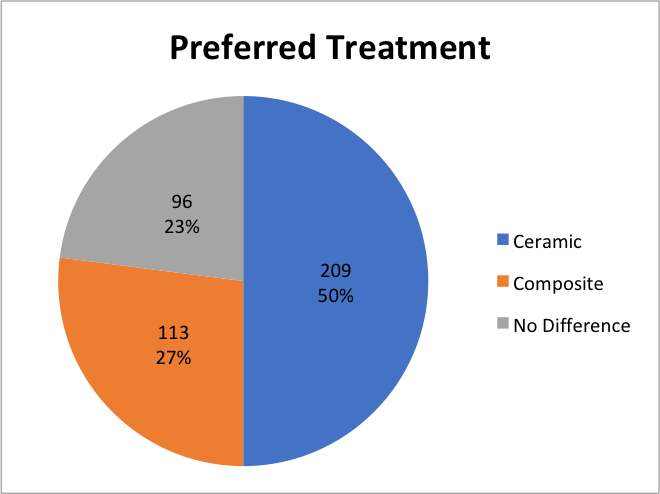
Precisely 50% of the sample population would use ceramic veneers on their patients in the same clinical circumstances. And 27% would prefer to use composite, whilst 23% stated they had no preference under the same clinical circumstances. These results give an overview that dentists would prefer to use ceramic when veneers are provided.
Short-term complications
In the short term, nearly half of the participants had found no difference in complications between composite or ceramic veneers (47%). Between the two materials however, composite was found to have the highest number of complications (40%) compared to ceramic, where only 13% had complications in the short term. Furthermore, in the short term, more dentists state there is no difference between the two types of restorative materials.
Long-term maintenance
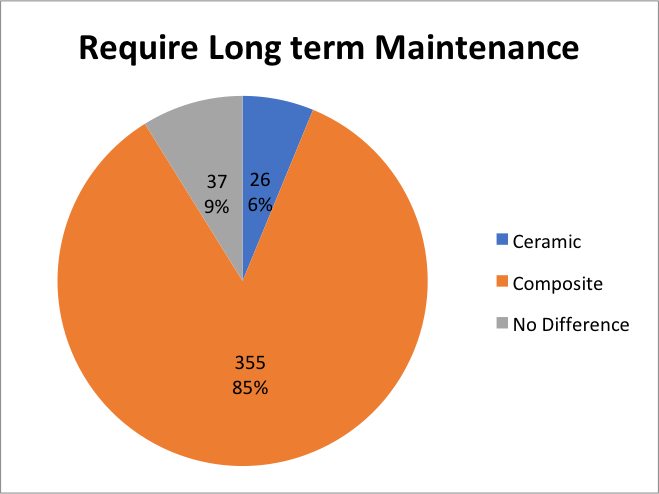
An overwhelming response found 85% of participants think composite requires more long-term maintenance compared to ceramic (6%). And 9% of the population surveyed found no difference between the two types of restorative material.
Aesthetic outcome
Aesthetics is subjective, and this questionnaire only focused on the dentist’s perspective, as we did not research the patient’s opinion on aesthetics.
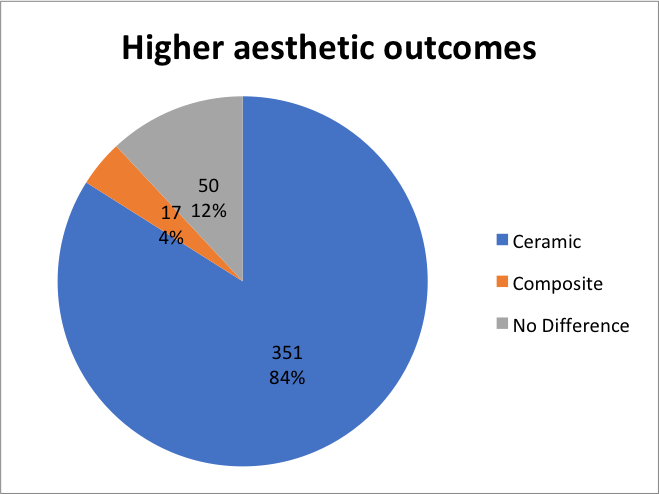
The data collected showed that out of a total sample size of 418, 351 dentists rated ceramic veneers as having the highest aesthetic outcome. This equates to 84% of the population sample favouring ceramic to composite in terms of aesthetic result.
Influence of patient’s age
Results show 77% of participants said the patient’s age had influenced them as to whether to provide composite or ceramic veneers. Surprisingly, still, 23% of respondents voted to state that the patient’s age has not influenced them providing the two types of restorative material. Patients must be appropriately informed when there is elective removal of healthy enamel and dentine, particularly in younger patients. We have a duty of candour to our patients when we have the potential to cause harm, particularly when we have seen the biological cost associated with ceramic veneers.
Patient demand
Results also show that 59% of the dentists that answered the survey feel there is more demand for composite veneers compared to ceramic in 2019. Interestingly, the demand for porcelain veneers is 15%.
Comparative results
Material of choice compared to number of years of experience
Across the data in all groups (1-5, 6-10, 11-15, 16-20, 21+ years qualified), ceramic is the clinicians preferred choice of material under the same clinical circumstances. The group with the highest number of participants selecting ceramic was the 1-5 years qualified group (64).
Short-term complications compared with the number of years qualified
Analysis of the data found a significant relationship between the number of years qualified and the short-term complications associated with the restorative materials.
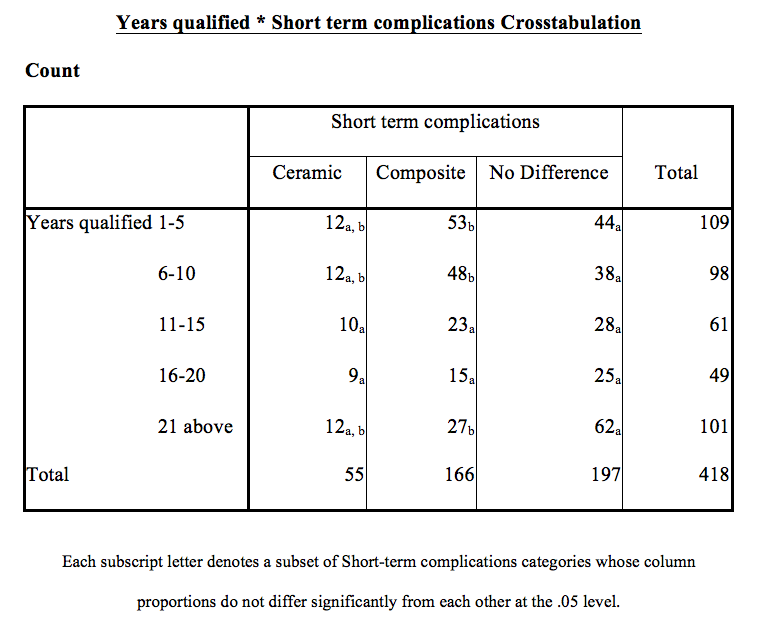
In the 1-5 years qualified group, 21% of respondents found short-term complications with ceramic, but 32% found post complications higher with composite.
As the subscript letter is different between ceramic and composite in this group, this means the result is significantly different in terms of proportion relative to the total for that column. The result also applies to the 6-10 years qualified group.
We used a chi-square test in SPSS (Version 22) to test the null hypothesis that the groups of the number of years qualified had equal short-term complications versus the alternative hypothesis that the proportions were not equal. The assumptions underlying the chi-square test were satisfied.
The test showed a significant result (p=0.016), so we reject the null hypothesis. We conclude that the number of years qualified can influence the short-term complication post-response.
Discussion
Material of preference
The study found that although ceramic veneers had the highest biological cost, clinicians still prefer this method of treatment, if patient finance was not a factor. This result is statistically significant (p=0.000). Therefore, the clinician would be comfortable to prepare the tooth in the majority of cases with the hope of increased restoration longevity and a higher aesthetic outcome. However, studies by Tyas (2004) concluded there is no such thing at the ‘ideal veneer’. There is no reliable evidence to show one type of veneer is better than the other (direct versus indirect) with regards to the longevity of the restoration (Tyas, 2004).
There was a relationship between the number of years qualified and the preferred restorative technique, although this result was not statistically significant. It showed that those dentists qualified within five years preferred ceramic veneers compared to composite veneers under the same clinical circumstances, if patient finance was not a factor. With a trend towards minimally invasive dentistry and minimal intervention taught at the undergraduate level, the results are surprising that in the 1-5 years qualified group, the preferred treatment option was ceramic veneers. Generally, dentists would accept that ceramic veneers would require some preparation, and therefore is this identifying a lack of experience in the 1-5 years qualified group?
Aesthetic outcome and patient demand
Results show 351 dentists rated ceramic veneers as having the highest aesthetic outcome. Precisely, 84% of the population sample favours ceramic to composite in terms of aesthetic result. Ceramic restorations do provide excellent aesthetics, and even though with modern-day composite materials and the advancement of dental technology, clinicians still prefer ceramic. However, dentists believe the patient demand for composite veneers (59%) are greater than ceramic veneers (15%) to improve aesthetics with minimal or no tooth preparation and their ability to be repaired when required. This stems from the patients ‘wants’ and is not necessarily what the patients need. Over time, composites lose their lustre and are more prone to staining compared with indirect ceramic veneers (Gresnigt, Kalk and Ozcan, 2013).
These results do not correlate with the study by Meijering et al (1997) where they found that dentists were unable to differentiate between composite or ceramic veneers. Even though after two years, the patients had a much higher level of aesthetic satisfaction towards porcelain veneers (p <0.05) (Gresnigt, Kalk and Ozcan, 2013).
Long-term maintenance
The majority of dentists (85%) find composite veneers require more long-term maintenance than ceramic veneers. This finding correlates to the study by Nalbandian and Millar (2009) that also states this. However this study focused on the patient’s opinion on cosmetic improvement with direct composite and porcelain veneers. Patients favoured porcelain, as they were concerned about the long-term maintenance (p < 0.863) required with composite veneers.
Influence of patient’s age
Younger patients have higher quantities of enamel, and therefore, every effort possible should be made to preserve this (Atsu, 2005). However, 64 dentists (20%) stated that the age of the patient has not affected their treatment decision and accept the higher biological cost of tooth preparation associated with ceramic veneers. This result was statistically significant (p=0.021). We have to question those dentists on how many replacement restorations a young patient would require during their lifetime and the on-going complications and costs associated with this.
Short-term complications
The majority of the population sample found that in the short-term, the complications between composite veneers and indirect ceramic veneers were similar (no difference).
However, for dentists less than five years qualified, a significant relationship was found in the number of dentists reporting higher amounts of short-term complications for each restorative material. This group of individuals found much higher levels of short-term complications with composite veneers compared to ceramic veneers (p=0.016). What this result tells us is that dentists with less experience suffer from higher complication rates with composite veneers soon after treatment is performed. This finding is in keeping with the Meijering (1998) study in which the authors observed the dimensional changes during veneering procedures on discoloured teeth.
At two-year follow up, the authors found a relative failure rate of 14 out of 69 direct composite veneers (20%). This was higher than indirect composite (6%) and indirect ceramic veneers (5%) (Meijering et al, 1998).Relative failure would be described as those restorations with fractures, chipping or dislodgement (Meijering et al, 1997). The results, therefore, imply that experience affects the short-term complications with composite veneers.
This could be because newly-qualified dentists lack the skills, procedural knowledge and technical skill to place composite veneers appropriately.
Conclusion
The findings of this paper highlighted under the same clinical circumstances, dentists preferred to place indirect ceramic veneers compared to composite veneers (p=0.000), irrespective of the number of years qualified. A postal questionnaire performed in 2008 with 662 responses found that the preferred choice of indirect restoration for anterior teeth was porcelain veneers (81%), with direct composite veneers only being preferred by 14% of the study sample (Brunton et al, 2012). We can see that almost 10 years later more dentists favour the use of composite veneers (27%). This could be due to improved education and material advances since the 2008 study was performed.
The study identified that 85% of dentists found composite veneers require more long-term maintenance compared to ceramic. This supports the findings of a review of the literature by Peumans et al (2000). They found that the maintenance of aesthetics of ceramic veneers in the medium to long term was excellent. Additionally, the incidences of short-term complications were greater with composite veneers. This was significantly influenced by the number of years qualified (p=0.016). The randomised split-mouth study by Gresnigt (2013) evaluated the clinical performance of composite veneers and ceramic veneers and measured outcomes such as chipping, fracture, debonding, and caries. Gresnigt found that surface quality changes were more frequent in composite veneers and therefore require more long-term maintenance in terms of polishing and repair of restorations (Gresnigt, Kalk and Ozcan, 2013).
Therefore, patients must be adequately informed of the maintenance required as well as the importance of regular reviews to assess the need for renovation or repair over time (Mackenzie et al, 2013). Therefore a protocol can be established for the assessment of renovation as well as the technical treatment to maintain these restorations over the patient’s restorative lifetime.
Results show 20% of dentists were not influenced by the patient’s age when providing ceramic veneers and accept the biological cost associated with such tooth preparation. The result was statistically significant (p=0.021). It has been documented that 3-30% of the coronal tooth structure is removed when providing indirect ceramic veneers (Edelhoff and Sorensen, 2002). It is concerning that 64 dentists in the study would be willing to provide indirect ceramic veneers on younger patients, knowing that tooth destruction has to take place to offer the treatment. This area needs to be researched further to see if dentists understand the consequences of tooth preparation on younger patients and the restorative cycle over the patient’s life.
A conclusion cannot be drawn as to which material performs better, as the evidence in the literature review is not reliable, and this was not the purpose of the research project.
Acknowledgements
The authors would like to thanks Dr Barry Quinn, department of restorative dentistry, Kings College London and Li-Ann Nalangan, statistician, and all the participants who completed the survey.
References
Atsu SS, Aka PS, Kucukesmen HC, Kilicarslan MA and Atakan C (2005) Age-related changes in tooth enamel as measured by electron microscopy: implications for porcelain laminate veneers. J Prosthet Dent 94(4): 336-41
Brunton PA, Sharif OM, Creanor S, Burke FJT and Wilson NHF (2012) Contemporary dental practice in the UK in 2008: indirect restorations and fixed prosthodontics. Br Dent J 212: 115-9
Burke F, Cheung SW, Mjör IA and Wilson NH (1999) Restoration longevity and analysis of reasons for the placement and replacement of restorations provided by vocational dental practitioners and their trainers in the United Kingdom. Quintessence Int 30(4): 234-42
Dietschi D and Devigus A (2011) Prefabricated composite veneers: historical perspectives, indications and clinical application. Eur J Esthet Dent 6: 178-87
Edelhoff D and Sorensen JA (2002) Tooth structure removal associated with various preparation designs for anterior teeth. J Prosthet Dent 87(5): 503-9
Gresnigt MM, Kalk W and Ozcan M (2013) Randomized clinical trial of indirect resin composite and ceramic veneers: up to 3-year follow-up. J Adhes Dent 15(2): 181-90
Kelleher M (2010) The ‘Daughter Test’ in aesthetic or cosmetic dentistry. Dental Update 37(1): 5-11
Mackenzie L, Parmar D, Shortall A and Burke FJT (2013) Direct anterior composites: a practical guide. Dental Update 40(4)
Meijering AC, Peters MC, DeLong R, Pintado MR and Creugers NH (1998) Dimensional changes during veneering procedures on discoloured teeth. J Dent 26(7): 569-76
Meijering AC, Roeters FJ, Mulder J and Creugers NH (1997) patients’ satisfaction with different types of veneer restorations. J Dent 25(6): 493-7
Nalbandian S and Millar BJ (2009) The effect of veneers on cosmetic improvement. Br Dent J 207: E3
Peumans M, Van Meerbeek B, Lambrechts P and Vanherle G (2000) Porcelain veneers: a review of the literature. J Dent 28(3): 163-77
Robinson R, Patel D and Pennycate R (2004) The Economics of Dental Care. Office of Health Economics
Smales RJ and Berekally TL (2007) Long-term survival of direct and indirect restorations placed for the treatment of advanced tooth wear. Eur J Prosthodont Restor Dent 15(1): 2-6
Tyas M (2004) Lack of reliable clinical evidence for or against direct and indirect veneers. Evid Based Dent 5: 43
Wakiaga J, Brunton P, Silikas N and Glenny AM (2004) Direct versus indirect veneer restorations for intrinsic dental stains. Cochrane Database Syst Rev (1): CD004347

