











Follow Dentistry.co.uk on Instagram to keep up with all the latest dental news and trends.
 In this month’s Endo Expert column, Kreena Patel explores the complexities involved with a third root in mandibular molars.
In this month’s Endo Expert column, Kreena Patel explores the complexities involved with a third root in mandibular molars.
The majority of mandibular molars have two roots (mesial and distal).
Sometimes, an extra ‘supernumerary’ or ‘third’ root is present.
This is important when considering endodontic treatment, because of the additional canal located within this root. However, it can also impact surgical procedures or orthodontics because these teeth are much more difficult to extract or move.
Terminology
- Radix entomolaris (RE): extra disto-lingual root
- Radix paramolaris (RP): extra mesio-buccal root.
Carabelli (1844) first described the presence of a third lingual root in mandibular molars in literature.
Bolk (1914, 1915) then named the teeth radix entomolaris or radix paramolaris according to where the extra root was located.
Figure and caption taken from Calberson et al (2007).
Aetiology
The aetiology of the extra root remains unclear. It may be related to external factors during tooth development or due to an atavistic gene or polygenetic system.
Incidence
Radix entomolaris can be found in the mandibular first, second and third molars, occurring least frequently in the second molar.
Radix entomolaris in mandibular first molars is more common in certain ethnic groups:
- African populations – roughly 3%
- Eurasian and Indian – 5-30%
- Indigenous populations (Chinese, Eskimo, American Indians) – 5-30%.
Radix paramolaris is rare and occurs much less frequently than radix entomolaris.
It occurs most commonly in mandibular third molars (2%) and has only rarely been reported in mandibular second molars.
Morphology
An additional root in a mandibular molar is nearly always associated with an increased number of cusps (tuberculum paramolare). However, the converse is not true and increased number of cusps does not always relate to an increased number of roots.
Scouting the cervical aspect of a tooth with periodontal probing can help in detecting the bulbosity of an additional root.
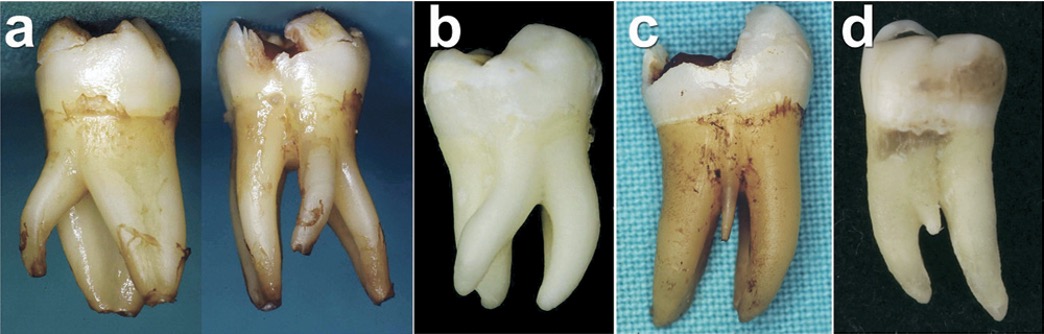
The extra root can be separate or partially fused with the other roots. Its morphology can vary from a short conical extension to one with a normal length (Figures 2 and 3). However, more often they are smaller than the other roots (Figure 4).
De Moor et al (2004) classified radix entomolaris on the root curvature:
- Type I: straight root canal
- Type II: initially curved entrance, which continues as a straight canal
- Type III: initial curved entrance with a second curve beginning in the middle and continuing to the apical third.
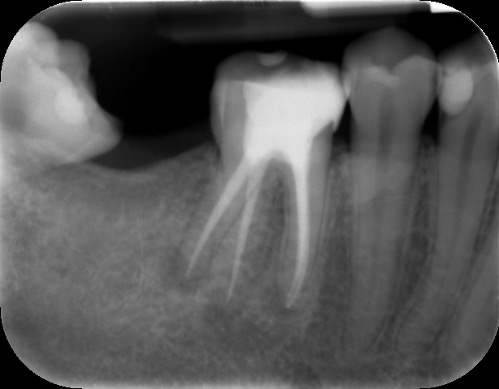
 Figure 3A: Radix entomolaris (LL6) with three roots and five canals. The main distal root (DB) can have two canals (DB1 and DB2) as well as the extra DL root; in this case the DB1 and DB2 joined in the mid third of the DB root. The DL root was a comparable length to the other roots. A) Preoperative radiograph
Figure 3A: Radix entomolaris (LL6) with three roots and five canals. The main distal root (DB) can have two canals (DB1 and DB2) as well as the extra DL root; in this case the DB1 and DB2 joined in the mid third of the DB root. The DL root was a comparable length to the other roots. A) Preoperative radiograph

Radiographs and CBCT
It is important to assess radiographs carefully for the presence of extra roots.
In radix entomolaris, the disto-lingual root often lies on the same bucco-lingual plane as the main distal root.
This superimposition can ‘hide’ the root, making it difficult to identify. Therefore, a parallax radiograph (taken from a 30 degree mesial or distal angulation) is helpful.
Three-dimensional imaging using CBCT is also very useful in identifying an additional root and treatment planning. It provides a ‘roadmap’ for endodontic treatment and highlights any curvatures present (Figure 5).
 Figure 5A: CBCT helps identify the number of roots and canals. It also allows us to visualise the degree and location of the curvature of the DL canal so treatment can be planned accordingly A) Periapical radiograph showing three roots present
Figure 5A: CBCT helps identify the number of roots and canals. It also allows us to visualise the degree and location of the curvature of the DL canal so treatment can be planned accordingly A) Periapical radiograph showing three roots present
Clinical advice
A detailed clinical and radiographic examination (as detailed above) are important to identify the presence of radix entomolaris or radix paramolaris (Figure 6).
 Figure 6A: Radix entomolaris LR6. Clinically LR6 had an extra cusp (tuberculum paramolare). Periodontal probing cervically revealed a slight bulbosity in the disto-lingual area indicating there may be an additional root present. The periapical radiograph showed an extra root (highlighted by the blue line)
Figure 6A: Radix entomolaris LR6. Clinically LR6 had an extra cusp (tuberculum paramolare). Periodontal probing cervically revealed a slight bulbosity in the disto-lingual area indicating there may be an additional root present. The periapical radiograph showed an extra root (highlighted by the blue line)
The importance of magnification and light cannot be emphasised enough when treating teeth with complex morphology.
The anatomy of the pulp floor is darker in colour. These dark dentine lines provide a helpful ‘map’ to guide the clinician to where the canal orifices are located. A long, sharp endodontic probe (DG16) can then be used to scout the entrance of the canals.
The access cavity will need extending in the direction of the extra canal (RE: disto-lingual or RP: mesio-buccal). A blunt-ended bur (such as an Endo-Z bur) is very useful to enlarge the access as required. Ultrasonics also provide a controlled and conservative way of refining the shape of the access cavity to allow straight line access.
The coronal part of the radix canal is often significantly curved. It is important to spend time coronally flaring to prevent creating a ledge here. I find the nickel titanium rotary orifice openers particularly useful for this (such as XA or SX by Dentsply Sirona).
Following this, the clinician can create a manual glide path using small hand files (up to a size 10).
The radix root is often narrow and curved coronally and/or apically.
Therefore, I prefer to avoid Gates Gliddens drills, which are fairly aggressive and could result in a strip perforation.
Similarly, larger stainless steel hand files are stiffer and can lead to canal transportation. I recommend using flexible nickel titanium instruments to shape after the initial glide path is formed.
The canal may need tackling in two or three sections if the instruments struggle to progress to length. Be careful not to push the files. This can result in ledge formation or file fracture.
In a radix entomolaris, the main distal root (DB) may still have two canals (DB1 & DB2) (Figure 5). The DB2 is more difficult to locate and can be hidden in the isthmus between DB1 and DL. It is often in close proximity to DB1.
Use fine ultrasonics to conservatively open the isthmus to search for this canal (Figure 7).
 Figure 7A: Radix entomolaris LR6 with five canals: DB1, DB2, DL, MB, ML. The tooth had previously been extirpated by the patient’s general dentist and referred for root canal treatment due to complex morphology. Master cone and postoperative radiograph. Five canals can be seen on the master cone radiograph, with DB1 and DB2 merging in the apical third
Figure 7A: Radix entomolaris LR6 with five canals: DB1, DB2, DL, MB, ML. The tooth had previously been extirpated by the patient’s general dentist and referred for root canal treatment due to complex morphology. Master cone and postoperative radiograph. Five canals can be seen on the master cone radiograph, with DB1 and DB2 merging in the apical third
Conclusion
Lower mandibular molars can have an additional root.
The term radix entomolarix refers to the presence of an extra disto-lingual root and radix paramolaris to an extra mesio-buccal root.
The endodontic management of these teeth is more challenging.
Use of parallax radiographs and CBCT is beneficial when diagnosing and treatment planning these cases.
The clinician should be aware the extra root may be shorter, narrow and curved. A modified technique is often necessary during access and instrumentation to avoid complications.
If you would like to learn more about endodontics follow Kreena on Facebook and Instagram @kreenaspecialistendodontics.
References
Calberson FL, De Moor RJ and Deroose CA (2007) The radix entomolaris and paramolaris: clinical approach in endodontics. J Endod 33(1): 58-63

