Follow Dentistry.co.uk on Instagram to keep up with all the latest dental news and trends.
In the first of a regular series of articles, Hannah Hook and Tina Aster give a dental student’s guide to antibiotics.
Over the last few decades, research has highlighted the concern that antibiotic resistance is becoming a worldwide problem and poses a major threat to public health. With the ongoing pandemic and the over-prescription of antibiotics, this risk is growing exponentially (Sanderson, 2020).
Therefore, more than ever as prescribers, we need to act responsibly. We need to ensure we understand what we are prescribing, why we are prescribing it and how to correctly prescribe.
Basic knowledge of pharmacology enables us to do this.
Within dentistry we use three main groups of antibiotics. We can categorise these by their mechanism of action (Figure 1).
This article will cover the mechanism of action of these groups and any associated warnings. Along with an easy guide on when to prescribe antibiotics.
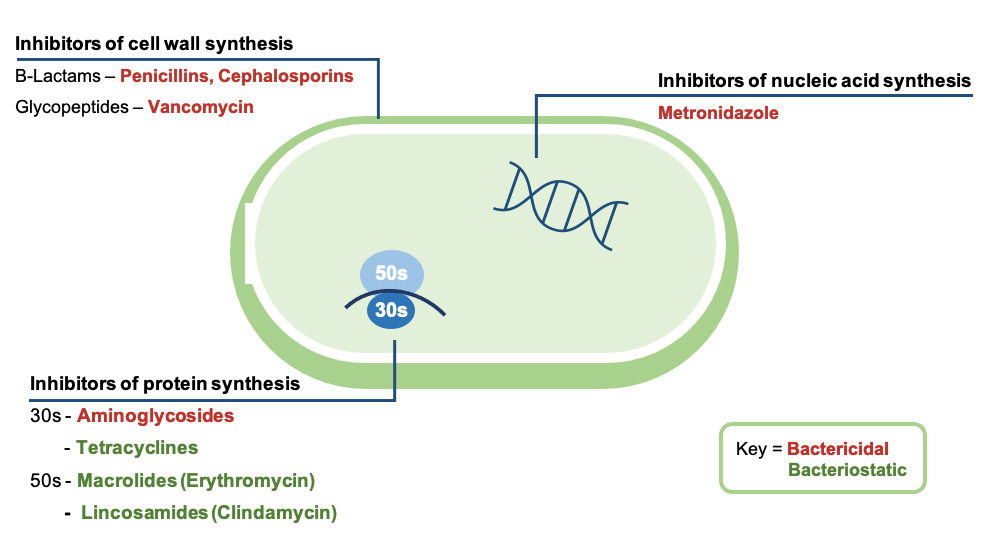
Inhibitors of cell wall synthesis
B-lactams and glycopeptide antibiotics disrupt the synthesis of the primary component of a bacterial cell wall – the peptidoglycan layer.
They irreversibly inhibit an important enzyme called transpeptidase. This prevents the cross linking of cell wall units. It results in a dysfunctional cell wall, which subsequently undergoes cell lysis and death; hence both types of antibiotics are bactericidal.
Warnings
- Approximately one in 15 people are allergic to antibiotics, especially penicillin and cephalosporins
- Penicillins can result in hypersensitivity reactions, including rashes and anaphylaxis and can cause diarrhoea
- Vancomycin can rarely cause ‘red man syndrome’, symptoms of which include a red rash involving the face, neck and upper torso.
Inhibitors of protein synthesis
Mechanism of action
Aminoglycosides and tetracyclines both inhibit the 30s subunit of ribosomes within a bacterial cell.
Aminoglycosides cause irreversible damage to the 30s subunit, preventing protein production and resulting in cell death. Therefore, it is bactericidal.
Tetracyclines, however, cause reversible damage, which slows down protein production without causing bacterial cell death. So it is bacteriostatic (Kohanski, Dwyer and Collins, 2010).
Similarly, macrolides and lincosamides are bacteriostatic as they cause reversible damage to the 50s subunit of ribosomes (Kohanski, Dwyer and Collins, 2010).
Warnings
- Tetracyclines are contraindicated in pregnant women and children under the age of 12, due to chelation of calcium ions into developing teeth and bones, which causes staining and occasionally dental hypoplasia
- Erythromycin potentiates the effect of midazolam and simvastatin. Do not use in combination with either
- Clindamycin can cause pseudomembranous colitis.
Inhibitors of nucleic acid synthesis
Mechanism of action
Bactericidal metronidazole is activated by oxidoreductase, an enzyme in anaerobic bacteria. It diffuses into bacterial cells and produces free radicals, which damages the bacterial DNA and ultimately results in cell death.
Warnings
- Avoid alcohol when taking metronidazole. If taken in combination a disulfiram-like reaction can occur. Symptoms of which include severe nausea and vomiting
- Other side effects of metronidazole are having diarrhoea or a metallic taste in the mouth
- Do not prescribe metronidazole for patients taking warfarin.
When to prescribe
Local measures first
When a patient attends in pain, where possible use local measures to resolve the issue.
For example, if pain is caused by a dental abscess, then options include; incision of soft tissue abscesses, access to root canals to relieve pus or extraction of the offending tooth.
In the case of pericoronitis debride and irrigate any areas of stagnation.
When necrotising ulcerative gingivitis/periodontitis (NUG/NUP) is present, local measures include scaling and oral hygiene instruction.
Justification of antibiotic prescription
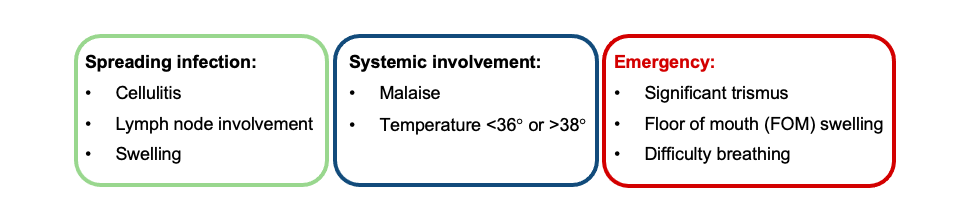
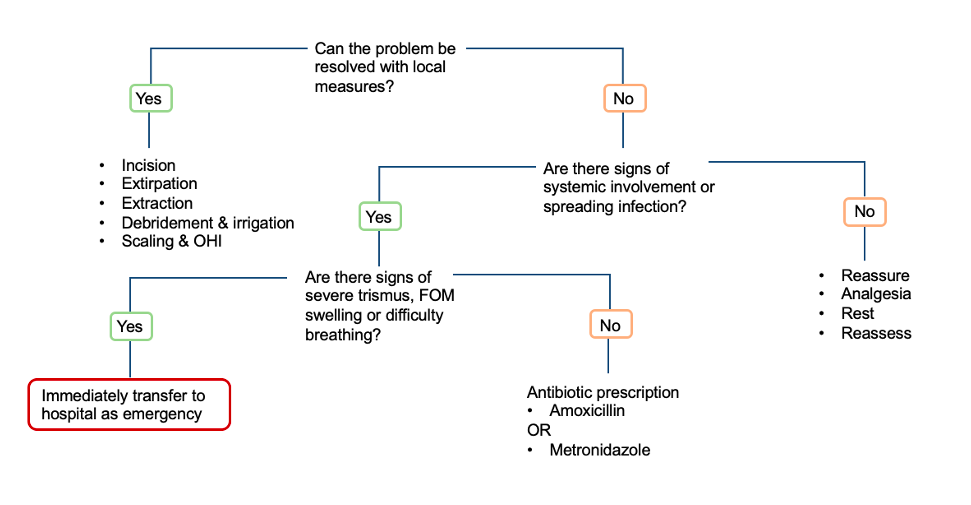
If local measures have failed or there is evidence of a spreading infection or systemic involvement (Table 1), consider an antibiotic prescription.
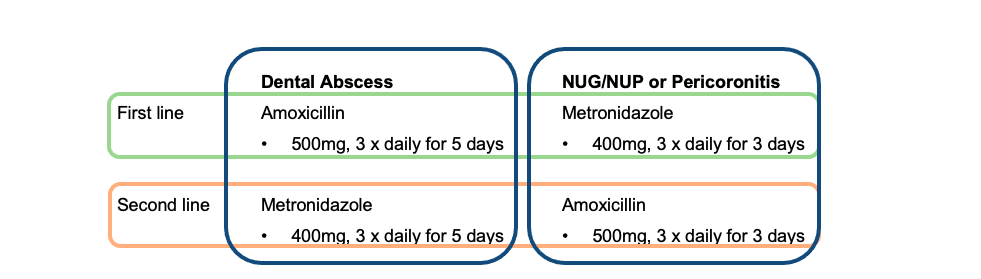
Prescribe first line antibiotics to target the problem. However if the first line antibiotic is contraindicated (allergy, pregnant, alcohol etc) then consider the alternative second line (Table 2).
The flow chart below can act as a useful tool when assessing the need for antibiotics (Figure 2).
Remember to only prescribe antibiotics if appropriate for the patient’s condition. Do not prescribe because you feel pressured by the patient to do so (Sanderson, 2020).
Don’t forget
If a patient has completed a course of antibiotics in the last six weeks, they are at an increased risk of harbouring bacteria resistant to that specific drug. Therefore, you should look at prescribing an alternative.
Also take care when prescribing for specific patient groups – such as the elderly, immunocompromised, pregnant or nursing mothers.
Similarly, consider if any modifications to doses are required for patients with renal or liver impairment. When in doubt, always check the British National Formulary!
Summary
- The main types of antibiotics used in dentistry work by either inhibition of cell wall synthesis, protein synthesis or nucleic acid synthesis
- Double check for any drug interactions or contra-indications when prescribing antibiotics
- Make sure you use local measures first, and prescribe antibiotics only when necessary and on a case-by-case basis.
References
Kohanski MA, Dwyer DJ and Collins JJ (2010) How antibiotics kill bacteria: From targets to networks. Nat Rev Microbiol 8: 423-35
Sanderson S (2020) Prescribing antibiotics for urgent dental care during the pandemic. Br Dent J 228: 749

