
 This month Kreena Patel explores the importance and differences between apex locators and their use in endodontics.
This month Kreena Patel explores the importance and differences between apex locators and their use in endodontics.
Complete removal of the pulp, necrotic tissue and microorganisms are critical for endodontic success. Accurate determination of working length is an essential part of the process.
The outcome of endodontic treatment is significantly lower if the root filling is long or short, or if it is not possible to achieve patency. Over-instrumentation can also lead to complications and postoperative pain.
This month I will discuss working length determination and the benefits of using electronic apex locators (EAL).
Anatomy
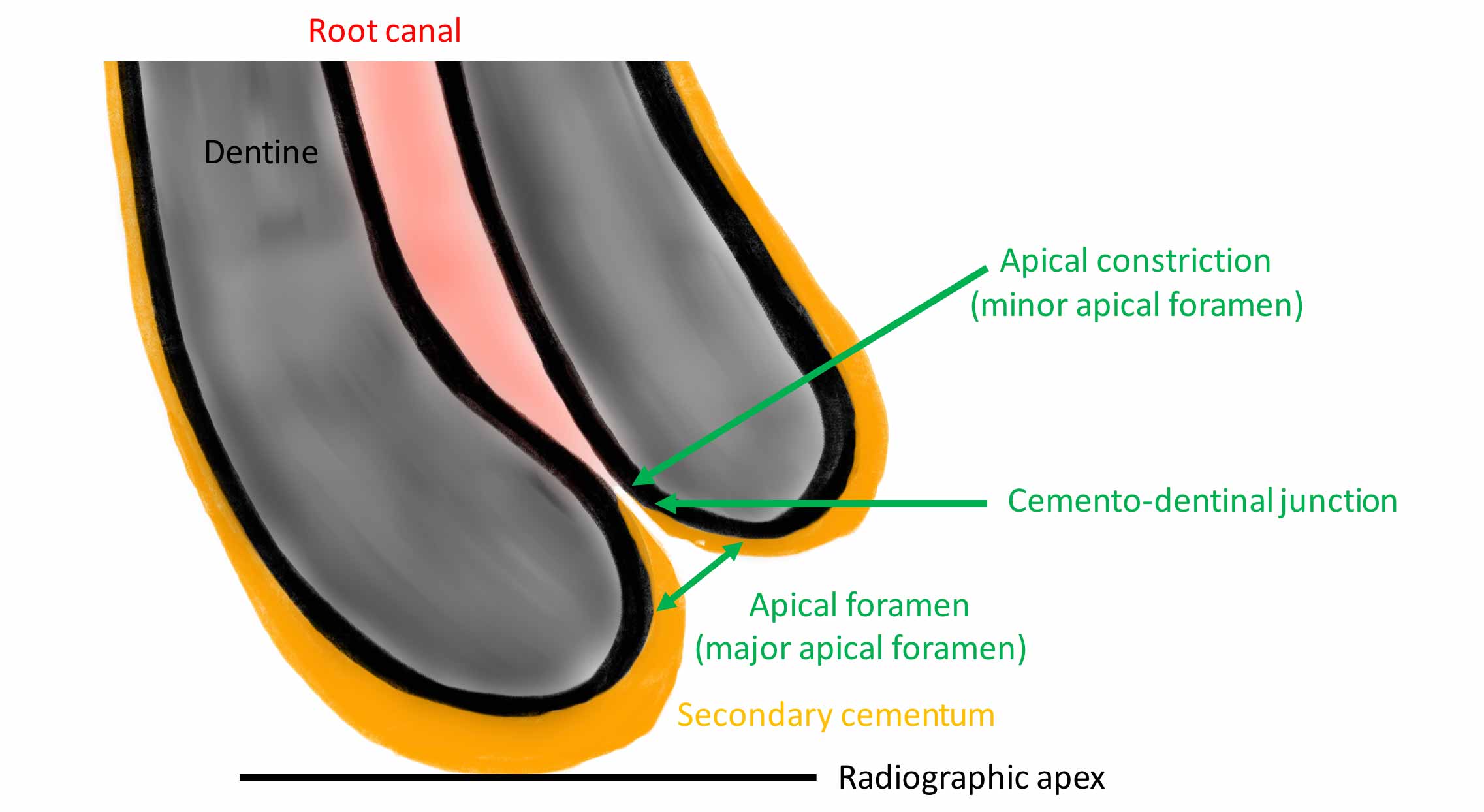
The narrowest part of the canal is the apical constriction or minor foramen. From this point the canal gradually widens to terminate at the apical foramen or major foramen (Figure 1).
The cemento-dentinal junction (CDJ) is the histological landmark where the pulp ends and the periodontal ligament starts. It is expected to lie at the apical constriction (AC) but it’s position can be irregular.
Working length
The working length (WL) is the length from a coronal reference point to the apical limit of the preparation. The optimal end point for root canal preparation and obturation is to the apical constriction. This in theory would create the smallest wound.
Methods to determine WL
- Radiographs: the apical constriction is estimated at 0.5 to 1mm short of the radiographic apex by anatomical studies. However, the location and form of the apical constriction are variable. Therefore we cannot determine its position accurately using radiographs
- Tactile sensation: we can sometimes detect the apical constriction using hand files. However, there has been shown to be substantial variation when using this method by even experienced clinicians. In addition, the canal may be sclerosed or the apical constriction may have been destroyed by inflammatory resorption
- Paper point technique: bleeding or exudate on the tip of a paper point can determine working length but this method is often unreliable
- Electronic apex locator (EAL).
Limitations of working length radiographs
- The apical foramen is not always located at root terminus (Figures 1 and 2). There can be up to 3mm variation in 50-98% of roots. It is generally greater in posterior teeth
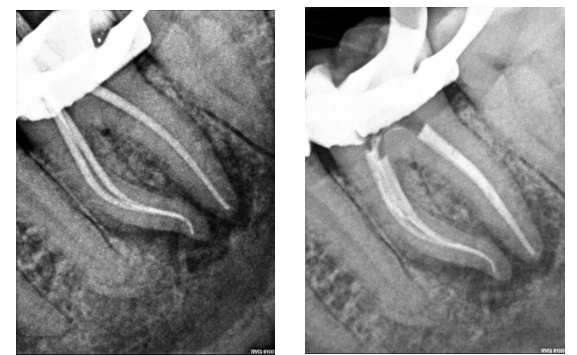
Figure 2a: Master cone radiograph. The apical foramen exits the root laterally on the mesial root. An apex locator is essential in these cases to determine the WL. b) Mid-fill radiograph - The distance between with apical constriction and root terminus increases with age due to secondary cementum deposition at the root apex (Figure 1)
- Dummer et al (1984) classified the apical constriction into four types (Figure 3). Estimating the working length using radiographs could lead to under-preparation of type B and over-preparation of type D
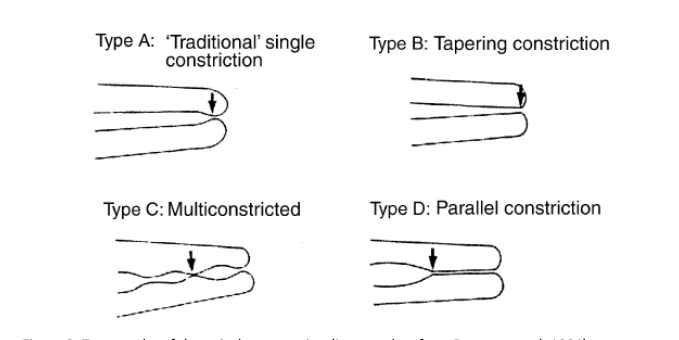
Figure 3: Topography of the apical construction (Image taken from Dummer et al, 1984) - Radiographs have several limitations that can cause difficulties and errors in WL determination
-
-
- Two dimensional: radiographs are two-dimensional images and offer a limited perspective particularly in the bucco-lingual plane (Figure 4)
 Figure 4a
Figure 4a
Figures 4: Radiographs are two-dimensional images offering a limited perspective in the bucco-lingual plane. This makes WL determination challenging in some cases. Root canal treatment LL6 Figure 4a) Preoperative radiograph. Figure 4b: Master cone radiograph. The four separate canals are terminating at different lengths. It would not have been possible to estimate this accurately using a preoperative radiograph, and an apex locator was essential. Figure 4c: Postoperative radiograph
- Anatomical noise: overlying anatomy can make it difficult to visualise the area of interest (Figure 5)

Figure 5: Anatomical noise. The zygomatic arch and sinus are overlying the apex of UL7 making it difficult to determine the working length radiographically. A reliable apex locator reading is essential in these cases - Geometric distortion: elongation and fore-shortening of the root. This is significantly reduced when a beam-aiming device (Figure 6).
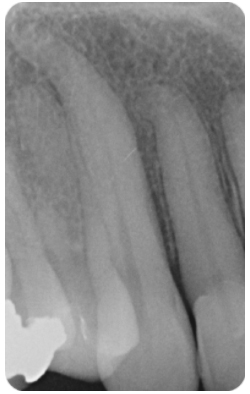
Figure 6: Geometric distortion. UR3: the root appears elongated where the film has been
pressed against the palate. Beam-aiming devices are essential in endodontics to limit the
effect of this but some degree of distortion is inevitable
- Two dimensional: radiographs are two-dimensional images and offer a limited perspective particularly in the bucco-lingual plane (Figure 4)
-
-


Electronic apex locators
Essentially, electronic apex locators work by using the body to complete an electrical circuit.
One side of the apex locator is connected to the oral mucosa (via a lip clip) and the other side to the file. The circuit is completed (zero reading reached) when the file contacts the periodontal tissue at the CDJ (Figure 1).
Brief history
Sunada (1962) found the electrical resistance between the mucous membrane and periodontium had a constant value (6.5kW).
The first generation (resistance based) apex locators use this value to determine the location of the apical constriction. Unfortunately, they were unreliable and would short-circuit when the file contacted pulp tissue, exudate, irrigating solutions or blood in the canal. They also used direct current and the patient sometimes felt a small electric shock sensation.
The second generation (impedance based) apex locators measured the opposition to the flow of alternating current or impedance. The design of these varied significantly and many needed to be individually calibrated to each tooth. However, they were still found to have variable accuracy, especially in wet canals.
To overcome these problems, the third generation apex locators used multiple frequencies. They require more advanced microprocessors to compute the complex mathematical algorithms.
The Root ZX (J.Morita) was the first self-calibrating third generation apex locator. It simultaneously measures two impedances at two frequencies (8kHz and 0.4kHz). It then calculates the level of the apical constriction using the ‘ratio method’. The Root ZX has been shown by numerous in vitro and in vivo studies to be accurate and reliable, despite the presence of fluid in the canal.
Fourth generation apex locators work in a similar way but measure one frequency at a time. They then use mathematical algorithms to assess the relationship between them. The manufacturers claim this improves accuracy but there is mixed evidence regarding this.

Advantages of apex locators
Apex locators have several advantages over other methods; they are easy to use, faster and can be used repeatedly without exposure to radiation.
I rarely need to take a WL radiograph, and usually move straight to the master cone radiograph. Verification of the length using at least one radiograph is essential prior to obturation.
When the position of the apical constriction is determined electronically, we are less likely to damage it by over-enlargement.
Apex locators also overcome the problems with radiographs discussed previously. Numerous studies have shown modern apex locators are more accurate than radiographs. However, this is dependent on the quality of the apex locator used.
There are numerous devices on the market and it is important to choose one that is reliable and you are comfortable using.
Apex locators are also particularly useful for diagnosing perforations, horizontal root fractures, and resorption. The apex locator will reach the zero reading as soon as the file contacts the periodontal tissue.
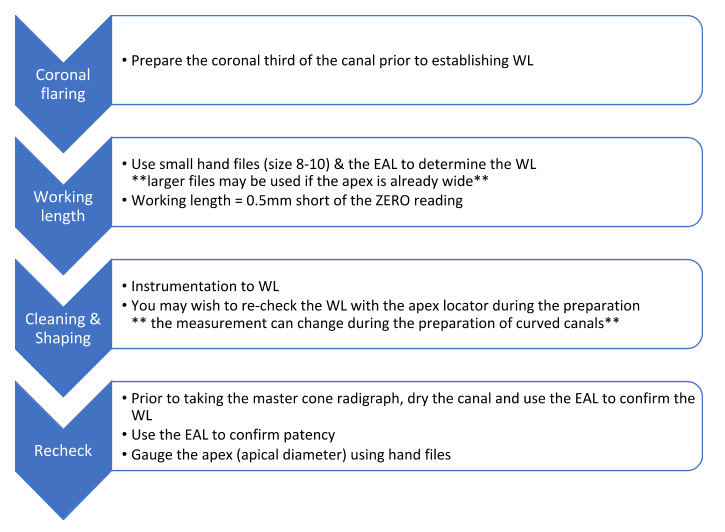
My protocol
I keep the apex locator connected and use it throughout the cleaning & shaping procedure.
Tips and troubleshooting when using apex locators
Coronal flaring
I recommend flaring the coronal third of the canal prior to trying to determine the working length.
Coronal flaring is useful for many reasons:
-
-
- The coronal aspect of the tooth is usually the most heavily contaminated. Disinfecting this space prior to placing files to full working length helps prevent pushing debris and bacteria further into canal or beyond the apex. This is a common cause of blockages, postoperative pain and infection
- You gain better tactile sensation from the tip of the file because it is no longer bound coronally. This helps with canal negotiation and reduces the strain placed on the file
- The working length measurement is less likely to change after coronal flaring because the canal curvature has been reduced.
-
Zero reading
The zero reading is the only accurate measurement produced by the apex locator. The visual scale bar leading to the zero reading does not accurately represent where the file lies within the canal.
However, this scale is helpful to check the reading is stable and moves in tandem with the file movements. If the zero reading flashes erratically then the reading is not accurate.
Metallic restorations
When the file contacts a metallic restoration (such as amalgam or metal crown) it will short-circuit the apex locator and give an inaccurate reading.
I prefer to strip the tooth of all restorations prior to carrying out root canal treatment, and place a pre-endodontic restoration using GIC or composite. In this way we can assess if there is any caries, microleakage or cracks and fully assess restorability.
If the restoration is not removed, it often helps to wrap PTFE tape around the coronal aspect of the file to prevent it contacting the metal restoration. A small piece of endo sponge may also help in the same way.
Dry the canal
Despite the advances in apex locators, fluid within the canal can sometimes interfere with the readings. It helps to dry the canal with a paper point if you are not able to get a consistent reading.
Excessive inflammatory exudate within the canal may cause reading errors. In this case, it is best to dress the canal with a calcium hydroxide medicament and recheck the WL at a subsequent visit.
Wide canals
Apex locators function best when the file contacts all the canal wall. Using larger files in wider canals can give a more accurate reading.
Low battery
Low voltages can make the EAL susceptible to errors.
Cardiovascular implantable electronic devices
Cardiovascular implantable electronic devices (CIED) or cardiac pacemakers are small lithium battery-powered devices.
They are surgically implanted beneath the skin, usually near the left clavicle, and have leads which run through the veins to the heart. They monitor heart rate continuously to detect arrhythmias and poor cardiac function. An impulse can be delivered to restore normal cardiac function when necessary.
There have been concerns with using apex locators in patients with these devices because the electromagnetic waves released could potentially interfere and disrupt the device.
Modern cardiac pacemakers have stainless steel or titanium covers, bipolar leads and capacitors. These protect and filter out electromagnetic interference.
The patient’s body (skin, muscle, fat, bone, teeth) also resists conduction of the electromagnetic currents and insulate the pacemaker from interference.
A recent systematic review, which includes in-vivo studies found apex locators could safely be used in patients with CIED. It is recommended to keep the EAL at least 10-20cm away from the CIED and its leads. Consultation with the patients cardiologist remains advisable.
Conclusion
Apex locators are easy to use, speed up treatment time and can also be used repeatedly without exposure to radiation.
They make root canal treatment more predictable and are an important part of the endodontic armamentarium.
References
Al Rahabi MK and Ghabbani HM (2019) Influence and safety of electronic apex locators in patients with cardiovascular implantable electronic devices: a systematic review. Libyan J Med
Ali R, Okechukwu NC, Brunton P and Nattress B (2013) An overview of electronic apex locators: part 2. Br Dent J 214(5): 227-31
Dummer PM, McGinn JH and Rees DG (1984) The position and topography of the apical canal constriction and apical foramen. Int Endod J 17(4): 192-8
Gordon MP and Chandler NP (2004) Electronic apex locators. Int Endod J 37(7): 425-37
Martins JN, Marques D, Mata A and Caramês J (2014) Clinical efficacy of electronic apex locators: systematic review. J Endod 40(6): 759-77
Ng YL, Mann V and Gulabivala K (2011) A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J 44(7): 583-609
Patel S, Dawood A, Whaites E and Pitt Ford T (2009) New dimensions in endodontic imaging: part 1. Conventional and alternative radiographic systems. Int Endod J 42(6): 447-62
Tsesis I, Blazer T, Ben-Izhack G, Taschieri S, Del Fabbro M, Corbella S and Rosen E (2015) The Precision of Electronic Apex Locators in Working Length Determination: A Systematic Review and Meta-analysis of the Literature. J Endod 41(11): 1818-23
If you would like to learn more about endodontics follow Kreena on Facebook and Instagram @kreenaspecialistendodontics.
Follow Dentistry Online on Instagram to keep up with all the latest dental news and trends.
- First
- Second
-
-
-
- Sub of Second
- Another Sub
-
- wfwfw
- wfwfw
-
-
- Third
- Fourth
-

