
 Josh Sharpling and Zo Ali explore toothwear, why patients may seek treatment and the different ways clinicians can help.
Josh Sharpling and Zo Ali explore toothwear, why patients may seek treatment and the different ways clinicians can help.
In the previous columns we introduced toothwear and how to recognise it.
Diagnosis is closely followed by stabilisation using dietary modifications, optimising eating habits, appropriate oral hygiene practices and working with the patient’s GP. Along with an occlusal splint, these interventions often form the mainstay of treatment for many patients.
There are, however, an increasing number of patients requiring intervention to restore either part or the entire dentition.
There are a number of reasons why a patient may require or request treatment. But broadly speaking, most complaints will relate in one form or another to aesthetics and/or function:
- Aesthetics
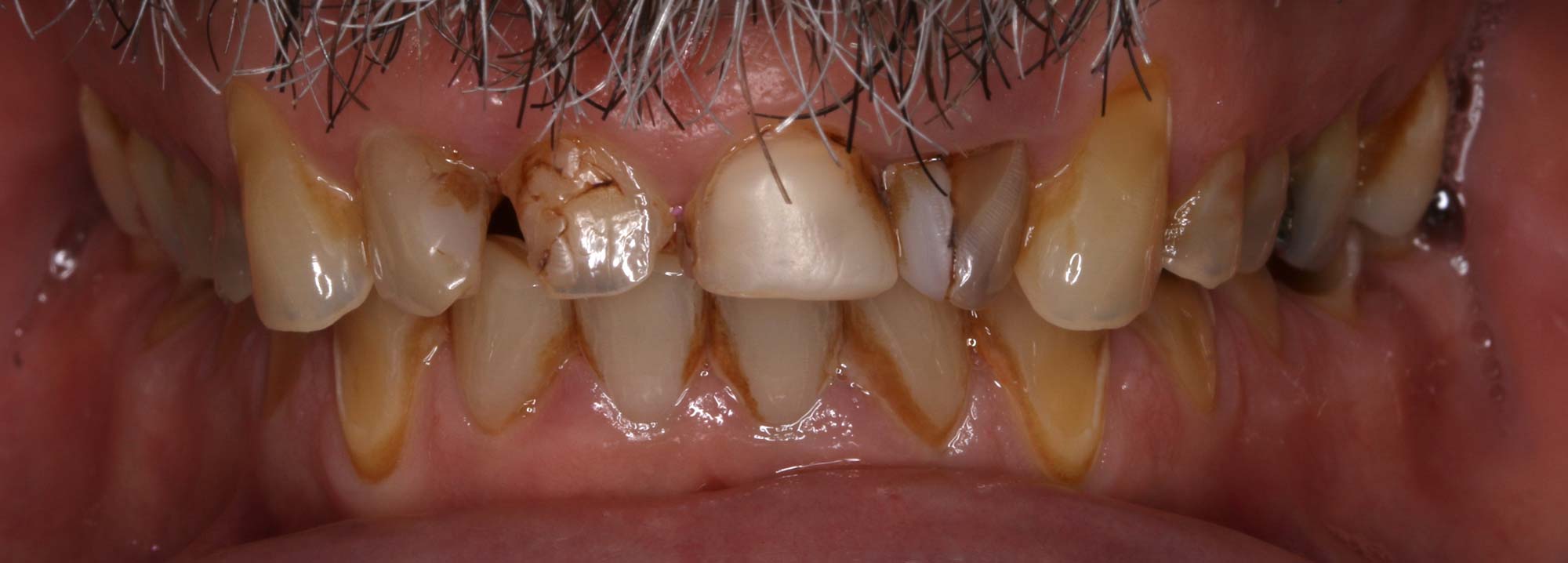
- This is one of the most common complaints that leads to restorative intervention. Frequently reported issues include reduced clinical crown height, lack of incisor when smiling and chipping or breaking maxillary incisor teeth (Figure 1)
- Dentine hypersensitivity (Figure 2)
- Uncontrolled, progressive toothwear virtually always exposes large areas of unprotected dentine. Further wear and the presence of acids leads to dentine hypersensitivity
- Whilst manageable for a few, most patients will find their quality of life affected by the restriction this condition imposes on their dietary habits. Others will have sensitivity even when brushing teeth. Those patients most severely affected experience pain even with atmospheric temperatures on a cold day
- Fractured teeth or restorations (Figure 3)
- As toothwear progresses, it can result in total loss of coronal structure. Either through gradual wear or through fracture as the toothwear process undermines the remaining enamel and dentine
- Wear of teeth responsible for mandibular guidance can also lead to fracture or other problems in posterior teeth. Wear of the guiding surfaces eventually leads to a lack of disclusion of the posterior dentition during excursive movements. The resultant contacts are, in most cases, interferences resulting in unfavourable loading. Where teeth are heavily restored, this often results in fracture. In untreated teeth, cracked tooth syndrome is becoming an increasingly common finding.


Treatment options
Irrespective of the presenting complaint, patients and clinicians will need to make a decision regarding treatment strategy.
Ultimately, this falls on the patient but as treating clinicians, we must ensure each patient is well informed regarding their personal presentation and prognosis. A partial rehabilitation is reasonable in some patients but entirely unsuitable for others.
It is the same with restorative materials; some patients will fair quite well with composite resin restorations. But the same treatment choices in another patient would be a total disaster.
Treatment options for individuals for erosive toothwear include orthodontics, crown lengthening and a multitude of prosthodontic approaches.
For the purposes of this discussion, we will consider only those patients who can be treated using prosthodontics alone and do not require input from other disciplines.
Reorganising the occlusion is a deliberate step that allows the predictable restoration of the patient’s dentition. A reorganised approach is required when the existing occlusal relationships are likely to result in premature failure of restorations or where space to place the restorations does not exist in the first place.
In most instances, but not all, this usually means increasing the occlusal vertical dimension to create interocclusal space and optimise occlusal design and aesthetics.
There are three main options when reorganising the occlusion. In order of increasing invasiveness and complexity:
- Dahl-type treatment
- Full-arch rehabilitation
- Full-mouth rehabilitation.
Dahl approach
This approach harnesses the compensatory capabilities of the various craniofacial components of the masticatory system.
Clinicians achieve relative axial movement of the teeth by purposely leaving restorations high in occlusion. It is generally indicated and limited to presentations involving localised wear of the anterior teeth.
Treatment involves restoration of the anterior teeth followed by a period of time up to 18 months. During this time, the posterior dentition is monitored for compensatory movements aiming to re-establish occlusal contacts.
It is generally successful but we cannot guarantee it. Seek patient consent for restorations on the posterior teeth where occlusal harmony is not achieved.
The only other instance where Dahl-type treatment is appropriate for generalised toothwear cases would be due to financial limitations.

Full-mouth rehabilitation
Generalised cases need treating with a full-mouth approach.
In these patients, virtually all of the teeth display signs of moderate to advanced wear. Treating only the anterior teeth would leave the posterior teeth with exposed dentine, often with associated pain and certainly at significant risk of increased wear.
This approach is very complex and requires diligent planning and execution. It also represents a significant financial commitment.
As such, many patients will opt for single arch treatment, ie a full arch rehabilitation. This usually means treating the maxillary arch and accepting the mandibular dentition without any drastic changes.
Stages in reorganising the occlusion
This is a short guide in the essential steps required to reorganise at an increased vertical dimension. By no means is this exhaustive and every clinician needs to have an extremely strong grasp of occlusal concepts before embarking on this kind of journey with any patient.
- Diagnosis, stabilisation and prevention
- Mounter study models in retruded axis position
- Diagnostic wax up at increased vertical dimension
- Production of stent based on diagnostic wax up
- Intra oral mock up using stent
- Definitive care.
The clinical procedures for the definitive restorations obviously vary greatly between materials, indirect and direct approaches, and even between clinicians.
Take great care at all stages of treatment to ensure a successful long-term outcome.
Follow Dentistry.co.uk on Instagram to keep up with all the latest dental news and trends.

