
Jameel Gardee and Jane Gosney talk through the smile makeover of a 24-year-old patient using digital fully guided workflows.
Digital dentistry is revolutionising the way we practise both in treatment planning and clinical execution. Digital fully guided workflows are offering practitioners more cost effective, precise, predictable and reproducible outcomes with less chair time than their traditional analogue workflows.
These benefits directly translate to the patient by offering shorter treatment times, eliminating the need for temporary restorations and offering true minimally invasive dentistry by the reduction of cumulative human error and operator sensitivity.
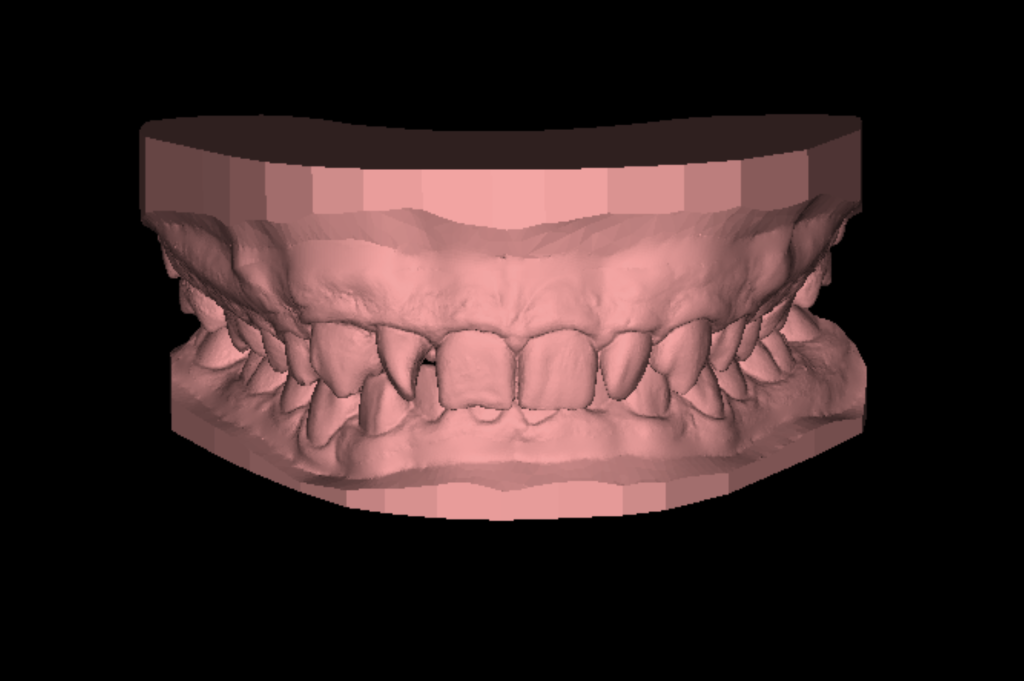
A 24-year-old patient presented for a consultation for a smile makeover. He was scheduled to travel abroad for 24 zirconia crowns but was seeking a second opinion before travelling (Figure 1 and 2).

Patient examination
A full comprehensive examination was completed including photographs, radiographs and digital intraoral scans. The patient had a gummy smile, crowded, worn and rotated teeth and a restricted envelope of function.
A functional assessment revealed no TMJ pain or symptoms. The patient detailed that he was a nocturnal grinder and that he occasionally wore a soft splint.

Treatment options
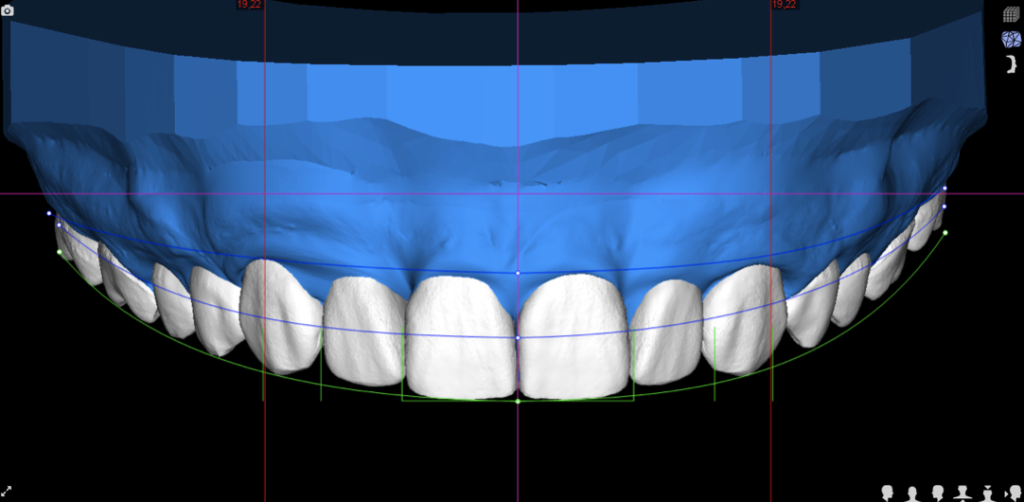
Starting with the end in mind and utilising facially guided dentistry principles, a digital smile design (DSD) was completed by DSDPlanning Centre Madrid (Figure 3). The additive digital wax up stl was printed in house and a motivational mock up putty stent subsequently made.
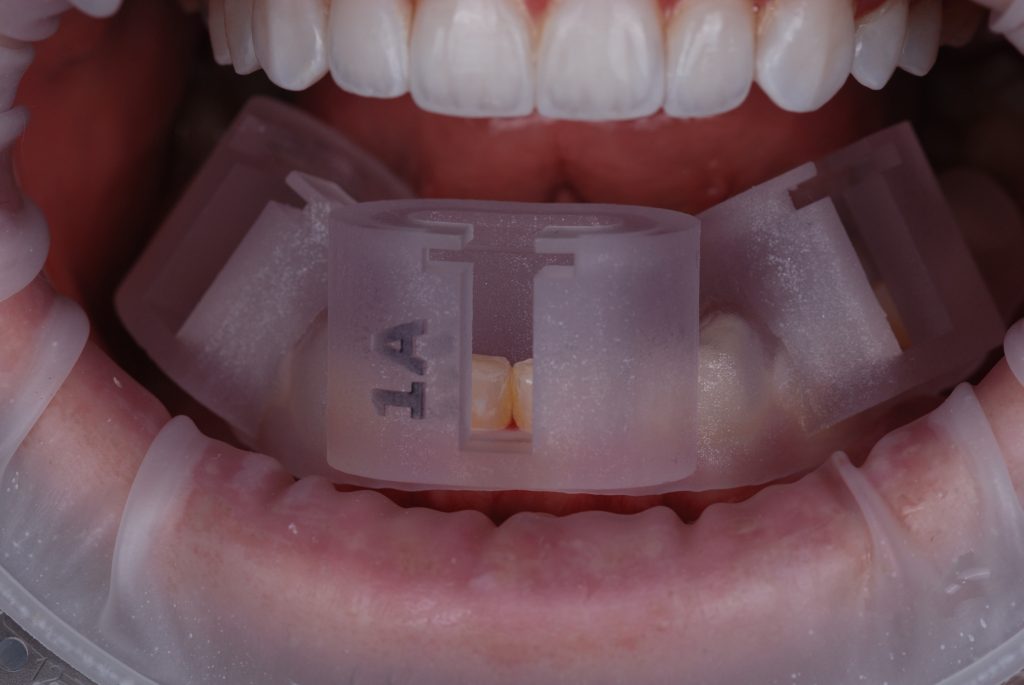
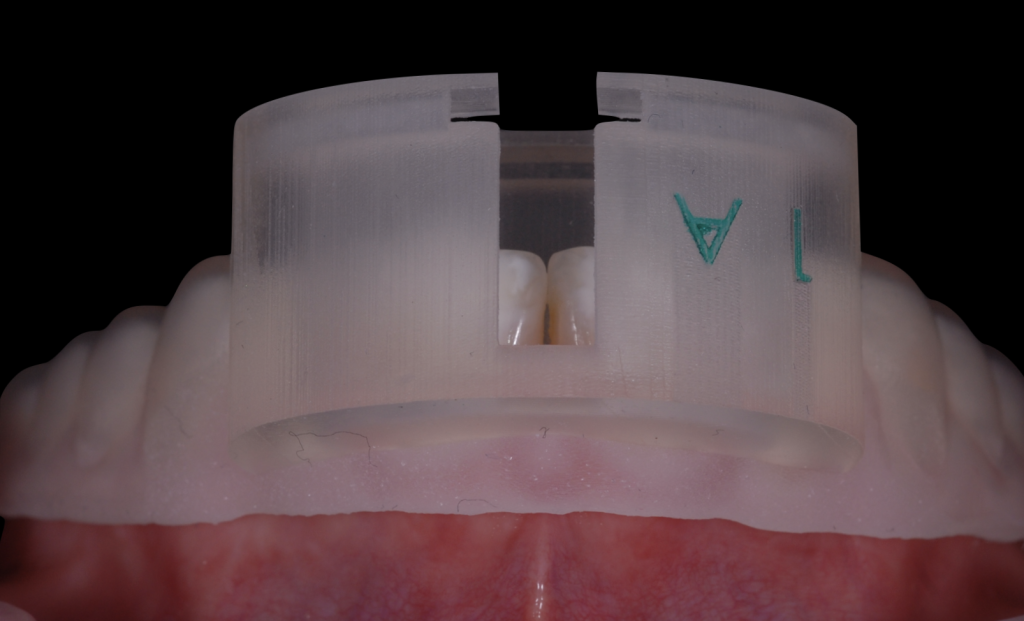
This trial smile was tried in the patients mouth with Luxatemp to confirm the proposed position and shape of his new smile (Figure 4). Presenting this visual aid to the patient enabled him to understand the ideal treatment pathway to achieve this aesthetic outcome – orthodontic treatment, gum correction surgery and restorative work.



Case planning and execution
The treatment plan was accepted by the patient and orthodontic treatment was completed with Invisalign (Figure 5 and 6). On completion, intraoral scans were retaken with the bite position recorded in CR and sent to Avant Garde Lab.
The initial DSD was adapted to the new tooth and bite positions using a virtual semi-adjustable articulator in Exocad in order create a functional digital wax up ensuring canine guidance with posterior disclusion in all excursions (Figure 7).


This biofunctional mockup was tested in the patient’s mouth with Luxatemp as a true reflection of the final planned position of the new restorations (Figure 8). On design acceptance from the patient, gingival recontouring was completed employing the mock up as a guide for the incisions in flapless crown lengthening with the Dentsurg Piezo from CV Dentus Brazil. After one week of healing, new scans were taken to reflect the new position of the gingiva and the DSD amended by Avant Garde Lab.
The patient was presented with material choices to achieve the desired shape and form of teeth and opted for lithium disilicate veneers and vonlays/tabletops to achieve the aesthetic requirements and increase in occlusal vertical dimension to achieve a stable functional position.
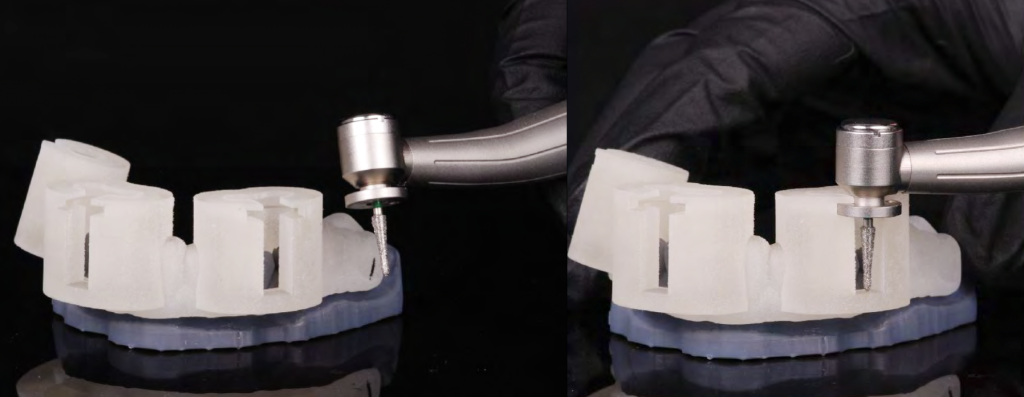
In order to maintain the most minimal preparations, reduce operator ‘over preparation’ and accurately replicate the pre-approved DSD the FirstFit fully guided digital tooth preparation system with its digitally planned reduction 3D printed guides, specialised handpiece and burs (Figure 9) was chosen to be utilised for the upper 5-5 and lower 5-5 with the lower 6s restorations to be Cerec milled in-house.
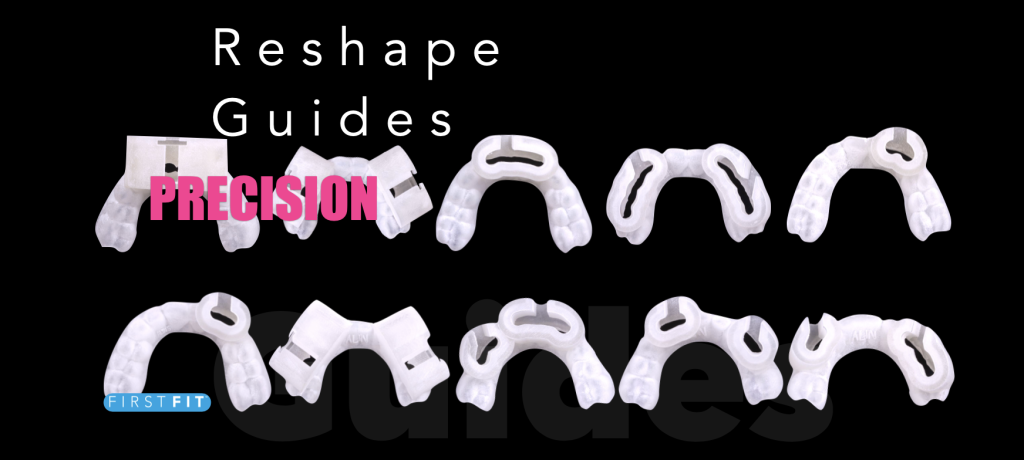
Shade BL3 was chosen and communicated to the lab with the AP Volution Shade guide (Figure 10). The case was delegated to FirstFit in Spain via the Avant Garde Lab which digitally designed the preparations of enamel necessary. 3D printed reshaping guides were manufactured to carry out the designed preparations in a controlled and highly accurate manner as described in our article in IJERD (1).





The final restorations were fabricated in pressed lithium disilicate and finished after cutback and layering (Figures 11 to 13).
The upper preparation guides, veneers and vonlays were delivered and in one visit the upper teeth were prepared (Figures 14 to 16) and the final restorations were cemented with a digital positioning tray (Figure 17) to aid seating. Cementation was completed with the manufacturers standard protocols (Figure 18).




This process was repeated for the lower teeth four weeks later (Figures 19 and 20) and the table top Emax CAD restorations for the lower 6s Cerec milled and cemented at the same time (Figure 21). The patient at five years post treatment complains of no issues (Figure 22).
Case discussion and reflections
The long term success of ceramic veneers has been directly correlated with enamel preservation (1) so a digitally planned and guided preparation system that allows us to prepare teeth in a controlled, minimally invasive and precise way severely reducing operator error in terms of over preparation such as FirstFit clearly has biological benefits.
FirstFit is more profitable to practitioners and more desirable to patients versus a traditional preparation technique as it improves chair time efficiency (time to prep and fit the upper teeth was approximately two hours), enhancing patient comfort and eliminating the need for temporary veneers.
FirstFit can also be adopted in a more traditional way for those practioners who wish it. It can be utilised for the preparation stage alone and the traditional impression/scan can be taken for fabrication at a second fit appointment.
Adopting a fully digital workflow from the beginning in this case allowed us to motivate the patient to proceed with a less aggressive treatment approach than the suggested 24 heavily prepped crowns abroad and also allowed for the delivery of a reproducible aesthetic result from the first mockup to the final result whilst mainitaining high control over function and occlusion.
New digital technology and workflows will continue to develop as research into robotics and fully guided systems continue and accessibility increases. It is of both of the authors’ views that ‘traditional’ analogue systems will soon be phased out completely and that comprehensive digital dentistry is modern dentistry.
Visit here for more information about Avant Garde Dentistry: First Fit Certification Course at the Avant Garde Residency www.avantgardedentistry.co.uk/the-residency.
Products used: AP solution shade guide, Sprintray 3D printer, Ivoclar (optragate, HF acid, Monobond plus, Adhese Universal, Variolink esthetic LC, Proxyt), Cerec.
References
- Laminate veneers: Preplanning and treatment using digital guided tooth preparation – J Esthet Restor Dent 2020 Mar;32(2):150-160
This article is sponsored by Avant Garde.

