Aligner Dental Academy presents a guide to diagnosing and treating dental crowding with clear aligner therapy.
Dental crowding is among the most prevalent orthodontic conditions, affecting up to 80% of patients in certain populations (Cenzato et al, 2021).
Crowding is as a discrepancy between tooth size and arch length. It may be generalised or localised and arises from multifactorial causes, including evolutionary jaw size reduction, altered muscle function, early tooth loss and mesial drift. Beyond aesthetics, it carries significant biological implications, contributing to plaque retention, caries, periodontal disease and occlusal dysfunction.
Invisalign offers a predictable, minimally invasive, clear aligner solution for managing crowding across the severity spectrum. This article outlines practical strategies for recognising, communicating, and treating dental crowding.

Classification and assessment
Crowding severity is commonly assessed by measuring the total displacement between adjacent contact points:
- Mild: 0-3 mm
- Moderate: 4-8 mm
- Severe: >8 mm (Golwalkar and Mistry, 2021).
Localised crowding may be more challenging to manage than an equivalent amount of generalised misalignment. A comprehensive evaluation, including intraoral scans, radiographs (where appropriate), periodontal assessment, and gingival biotype, is essential before initiating Invisalign therapy.
Biological and biomechanical strategies for space creation
Successful correction of crowding depends on creating adequate intra-arch space. Four main strategies exist: expansion, interproximal reduction (IPR), distalisation, and extraction.
Expansion
Arch expansion may be achieved anteriorly (through controlled proclination) or posteriorly (via buccal uprighting of premolars). Invisalign can predictably achieve up to 2mm expansion per quadrant in suitable periodontal conditions (Ma and Wang, 2023).
The gingival biotype must guide treatment planning: thin biotypes are prone to recession, whereas thicker tissues allow greater flexibility (Frost et al, 2023).
Excessive expansion, particularly in patients with thin biotypes, risks dehiscence or gingival recession.
Interproximal Reduction (IPR)
IPR involves selective enamel removal, up to 0.3mm per contact anteriorly and 0.5mm posteriorly, to create space while maintaining enamel integrity. IPR can also improve contact morphology and reduce black-triangle formation.
Distalisation
Sequential distalisation of posterior teeth (up to 3-4mm) can be predictably achieved with Invisalign Comprehensive, provided third molars are absent. The use of Class II elastics enhances anchorage and stability during distal movement. Papadimitriou et al (2018) concluded that Invisalign is highly effective for mild-to-moderate anterior crowding and molar distalization.
Extractions
In selected Class III or severe anterior crowding cases, lower incisor extraction may be indicated. Criteria include moderate-to-severe crowding, anterior crossbite, or mandibular tooth-size excess (Zhylich and Suri, 2011).
Proper staging, torque control, and the use of vertical rectangular attachments aid space closure and maintain alignment.
For Complex malocclusions, Hybrid or fixed mechanics may still provide superior control.
To access this resource, you need to be an Aligner Dental Academy member. If you aren’t already a member, please register here.

Clinical protocol for crowding
1. Diagnosis and planning
Detailed diagnostic records, including 3D scans and radiographs, where appropriate, are required to assess skeletal relationships and alveolar limits.
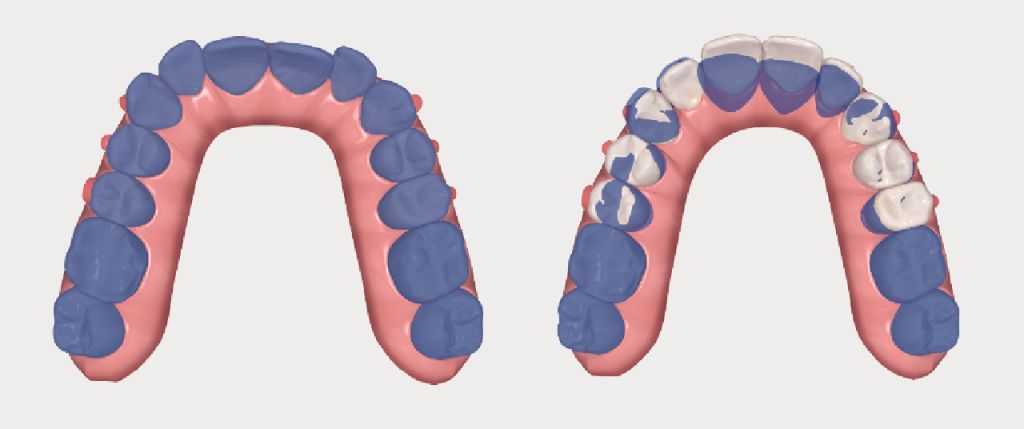
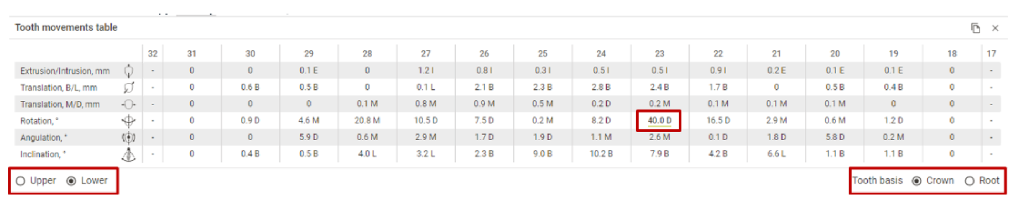
A precise ClinCheck setup is vital to outcome predictability. Several digital tools within Invisalign software assist clinicians, like the superimposition tool (for predicted versus actual expansion for feasibility), Bolton analysis tool (quantifies tooth-size discrepancies for accurate IPR planning), tooth movement table (displays per-tooth displacement to plan sequential staging), grid tool (measures planned expansion, intrusion, and overbite changes), etc.
Boston analysis tool
2. Monitoring and refinement
Patients must wear aligners 20 to 22 hours daily, changing every seven to 14 days. Clinical reviews every six to eight weeks allow monitoring of underperforming movements and planning of refinement stages.
3. Retention
Post-treatment, Vivera retainers are recommended full-time for six months, then nightly thereafter to prevent relapse.
To access this resource, you need to be an Aligner Dental Academy member. If you aren’t already a member, please register here.
Conclusion
Invisalign is a reliable and evidence-based solution for treating dental crowding. Predictable results rely on accurate diagnosis, sound biomechanical planning, and strong patient compliance.
Although fixed appliances retain advantages in complex three-dimensional movements, technological advances in aligner materials and digital simulation are narrowing this gap. With careful case selection and realistic expectations, Invisalign provides a biologically safe and aesthetic approach to long-term orthodontic stability.
Join Aligner Dental Academy live at its 2026 Symposium! For more details click here.
Look out for volume one of the Clear Aligner Essentials Guide, only available with Dentistry magazine November/December.
References
- Cenzato N et al, Prevalence of Dental Malocclusions in Different Geographical Areas: Scoping Review. Dentistry Journal. 2021
- Golwalkar, S A and Mistry, K M, (2021) Evaluation of dental crowding in relation to crown widths and arch dimensions. J Clin Orthod.
- Ma, S. and Wang, Y. (2023) Clinical outcomes of arch expansion with Invisalign. BMC Oral Health.
- Frost, N A et al, 2023, Periodontal biotype and gingival thickness in relation to buccal plate integrity. J Periodontol.
- Papadimitriou, A et al (2018) Clinical effectiveness of Invisalign orthodontic treatment. Prog Orthod.
- Zhylich, D and Suri, S (2011) Mandibular incisor extraction: a systematic review. J Orthod.
This article is sponsored by Aligner Dental Academy.

