
Ian Buckle describes the enormous responsibility placed on dentists in certain circumstances and talks about the risks and remunerations of making hugely important decisions for your patients.
One of the most common questions that we are asked during case presentation is ‘What would you do?’ This question places great responsibility on the dentist to answer very carefully and very honestly.
Sometimes the answer is very obvious but sometimes it is difficult. What are the risks? What are the rewards? What would you do?
Dulcie’s story

Dulcie was born with a very rare genetic disorder called Incontinentia Pigmenti (IP). At six weeks old her parents were told that she might go blind, deaf, be mentally retarded, her skull might not grow. These were just some of the things that might happen. Nothing could be done. They had just to travel hopefully. IP is a neurocutaneous disorder that affects the nerves and skin. Signs and symptoms can include hair loss (alopecia) affecting the scalp and other parts of the body, dental abnormalities (such as small teeth or few teeth), eye abnormalities that can lead to vision loss, and lined or pitted fingernails and toenails. Associated problems can include delayed development or intellectual disability, seizures, and other neurological problems.
As the years passed things got better. Dulcie’s skin improved although there were some patches of hypopigmentation. Her eyesight was fine, she was very bright and many of the problems that could have happened never materialised. There was only one problem – her teeth. As predicted some were missing and some were misshapen. Her deciduous teeth weren’t so much of a problem. She could eat okay and she looked cute with her little teeth. The eruption of her permanent teeth was delayed as often happens with IP. When the lower anteriors emerged they were conical. Not too much of a problem but other children can be very unkind. She was teased at school about her ‘Dracula teeth’. Her dentist did some bonding to make them a little more tooth shaped. The upper centrals weren’t too bad, the upper laterals were missing and the upper canines were very conical. When she was old enough an OPG was taken and it was discovered that she had multiple missing teeth.

So what’s all this got to do with case acceptance and ‘what would you do’? Well I have two connections to Dulcie. I am both her dentist and her father.
Our story
Holding any beautiful six-week-old baby in you arms and contemplating what their future might hold can be both wondrous and slightly scary. Faced with what we had just been told I think my wife and I were more scared than anything else. I have a feeling Dulcie wasn’t too concerned at that stage! After a few weeks of being slightly shocked things became normal. But I’m a fixer. I like to fix things. We’d been told to wait and see, but I needed to do something.
What could I do? I’ve always tried to do a good honest job and provide the best care I could for my patients. Now this had moved to a whole different level. This was personal! I knew that Dulcie might have tooth problems later so I set out to find the best dentists I could who could take care of my daughter should she need it. There is an old Japanese saying, ‘When the student is ready, the teacher appears’. It happened to me.
Cosmetic dentistry
Around this time, dentistry was just about to be hit by the cosmetic wave. Porcelain was the cure for everything and many of our patients seemed to be porcelain deficient! I knew that Dulcie might need some help with her smile so I needed to find out more. I went to listen to most of the cosmetic gurus of the time, most notably Larry Rosenthal. Larry was very good at two things: he was a real smile artist and a fabulous motivator. He encouraged you to be the best you can be and that if you were willing to learn and put in the hard yards you could be whatever you wanted to be. Larry may have his faults but I will always be grateful to him for this.
However, creating beautiful smiles asked as many questions as it solved, if not more. Would it last? How did you manage the occlusion? Did you really need so much tooth preparation?
Complete dentistry
I was lucky. Before I had engaged with cosmetic dentistry I had been to a lecture entitled ‘The Cosmetic-Occlusal Connection’ by John Cranham. John was the first person I had seen who showed excellent dentistry performed in a predictable, efficient manner. He showed that there was a balance between function and aesthetics, biology and structure that we needed to achieve if we were to create beautiful, long-lasting restorations. He also had a philosophy that I liked. We needed to develop a healthy work-life balance and we needed to act in the best interests of our patients.
John became my mentor. I discovered that he had learnt about complete dentistry from the dental legend, Dr Peter Dawson so I travelled to Florida and took all the courses at the Dawson Academy. That was when I first saw the acronym WIDIOM – would I do it on me?
So what about Dulcie?
Dulcie was getting older. We needed to start developing a plan for her long-term dental future. Orthodontics is an incredibly important part of complete dentistry and positioning Dulcie’s teeth so they could be restored minimally, aesthetically and functionally was going to be crucial to obtaining an optimum result. However, trying to find an orthodontist that would work to the same goals that I wanted to achieve was not easy. The goals of complete dentistry are to create beautiful, functional, healthy smiles that last – with the minimum amount of dentistry. To do this we would need a group of dentists who are looking to pursue the same goals. A real interdisciplinary approach, not a multidisciplinary approach.

Carl Roy, John Cranham’s orthodontist, introduced me to Domingo Martin from San Sebastián, Spain. Domingo is a director of the FACE (Roth Williams) group. He is a fabulous orthodontist and a very charismatic teacher. The FACE group has largely the same goals for their orthodontic treatment as I do for restorative care. Together with our periodontist/implant dentist, Inigo de Sada, we developed a plan that would give Dulcie a smile to be proud of.
Where we are today
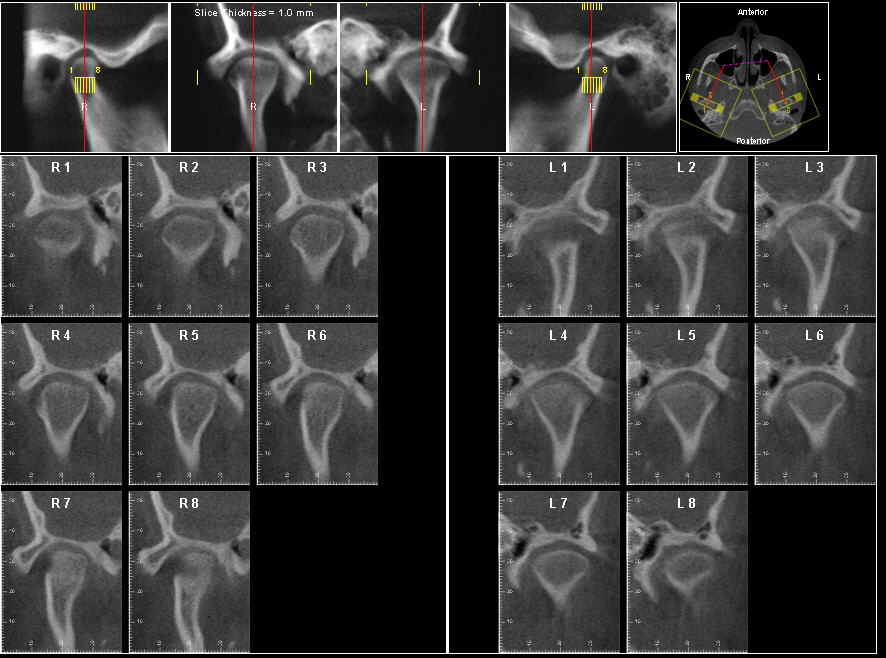
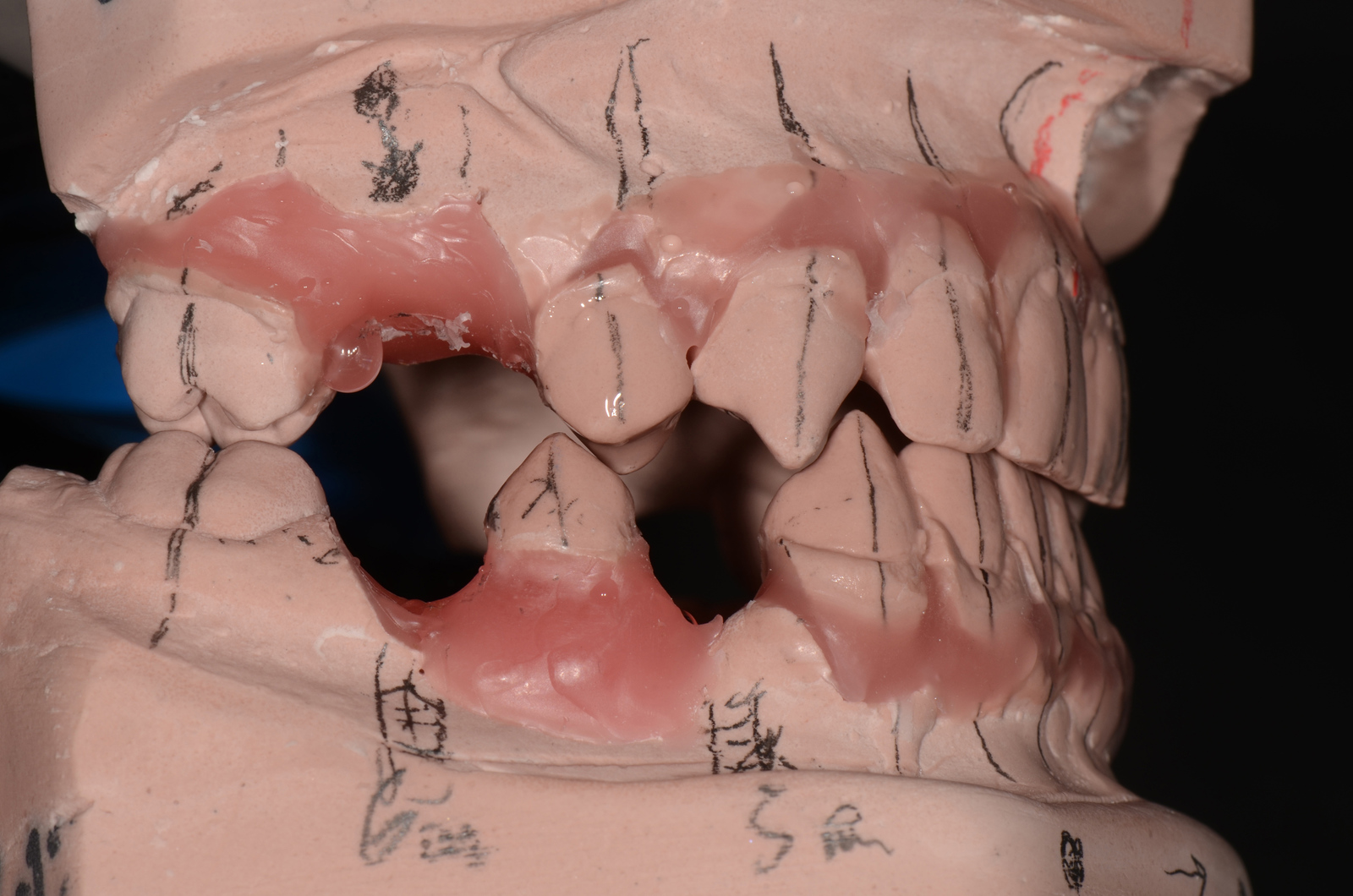
After careful examination and diagnosis, a diagnostic set up was created. Directed by the diagnostic set up, Domingo began to move the teeth to the matrix that we had designed. After a while Inigo was able to place some of the implants that would be required both to begin the restorative process and also to be used as anchorage for the orthodontics. We are getting there and we have a clear vision about what we want to achieve. Not for us but for our patient, Dulcie. Did she ask for healthy teeth that would last a lifetime? She’s a 19-year-old girl. She just wants a beautiful smile! Should she expect us as a team of professionals to deliver health and longevity? Absolutely!
So WIDIOM?
As you can tell this started as a very selfish journey but it has turned in to something bigger. The people that I have met along the way have inspired me to be the best I can be. More than that they have helped and encouraged me to improve. Through them I became involved in teaching which is incredibly stimulating. Not only is it huge fun and a tremendous challenge to share knowledge and experience with others but it is the best way to find out if you really understand something yourself. It’s a very humbling experience and inspires you to be a lifelong student.
In our practice we endeavour to treat patients the way we would like to be treated ourselves. We begin with a complete examination and from there help our patients to understand how we can help them to keep their masticatory system in good health and looking great for the rest of their life at a level that is suited to the individual. It can be challenging particularly when you are trying to solve complex problems with the least amount of dentistry. Many of these cases involve combined orthodontics, restorative, periodontal care and implants. After many years of searching, I have now assembled my ‘dream team’. Alberto Canabez from the FACE orthodontic group has joined me as has Inigo de Sada, periodontist and implantologist, who placed my daughter’s implants.
So when my patients ask me ‘What would you do?’ it is very difficult not to suggest the level of care that I have wanted for my daughter. Does everybody want that level of care? Not always. Life is full compromises. Sometimes it’s just not the right time. In these cases my goal is to keep my patients healthy and dentally happy until the time is right for them. At the same time I never want to carry out a treatment that will prevent us from providing optimal care in the future. But I always let my patients know what’s available and what their options are. What the risks are and what the rewards might be. Then I let them decide.

It never ceases to amaze me what patients will do to achieve their desired goals when you take the time to listen and explain. And if they do ask me ‘What would you do?’ I can honestly say that I will offer them the same care that I have chosen for my daughter.
For more information visit www.bdseminars.com.

